Introduction
Prostate cancer (PCa) accounts for more than 20% of newly diagnosed cancer cases and continues to be the second cause of cancer death in American men in 2020 [1]. Although PCa is only the fourth most prevalent malignancies in Chinese men, the total number of Chinese patients is still large owing to the huge population size and aging society [2]. Attributed to the adoption of early screening, the trend of clinical stage migration towards localized PCa has been witnessed, resulting in the survival improvement in Chinese patients [3].
Nonetheless, of the patients with localized PCa undergoing radical prostatectomy (RP) or radiotherapy, around 27% and 53% will develop a rising prostate specific antigen (PSA) which is defined as biochemical recurrence (BCR) [4]. Once BCR has been confirmed, the disease is at an overwhelmingly increased risk of incurable distant metastases and overall mortality [5,6]. Hence it is of great importance to early identify the patients at risk of BCR for timely intervention.
Circulating tumor DNA (ctDNA) shed by tumor cells into bloodstream is highly specific and sensitive to reflect the genomic profile of the tumor without invasive biopsies [7–9]. Multiple recent studies have validated the prognostic value of ctDNA in predicting clinical outcomes and monitoring treatment response across distinct solid malignancies [10–15]. Especially, the detection of ctDNA in the perioperative period is strongly associated with increased risk of disease recurrence and progression [16,17]. However, it still remains unknown if the early detection of ctDNA before primary tumor surgery could predict the disease recurrence in PCa.
Thus, in this work, we reported the results of a biomarker study in patients with non-metastatic PCa (nmPCa), where the main objective was to elucidate the association between the detection of pre-operative ctDNA and the risk of disease recurrence.
Materials and Methods
1. Patients and samples
We conducted a retrospective study of 161 patients with nmPCa, who were treated at the Ren Ji Hospital (Shanghai, China). The study was approved by the Committee for Ethics of Ren Ji Hospital (approval number: KY2019-081) and informed consent was obtained from each patient. Peripheral blood samples were collected before surgical intervention from 139 patients. Biopsied tumor tissue samples were collected from 31 patients. All the samples were collected at the time of diagnosis and all the studied patients were treatment-naïve. As the sequencing platforms updated over time, two different multigene panels were included in the present study. Two different platforms had the same detection sensitivity, which was validated in our previous study [18].
2. Targeted gene sequencing and bioinformatics
Targeted gene sequencing of all collected samples was performed at GloriousMed Clinical Laboratory (Shanghai) Co., Ltd. Sequence data analysis, including identification of germline mutation, somatic mutation, copy number variant, and quality control, were performed as described in Supplementary Methods. Deleterious alterations were called when they were nonsense/stop-gains, frameshift insertions and deletions, and ±1, 2 splice-site variants, or were previously reported as pathogenic or likely pathogenic in the ClinVar database.
3. ctDNA fraction estimating
The mutant allele fraction (MAF) was first calculated using the somatic mutation profile from the sequencing data, followed by a correction model [19]. ctDNA fraction was defined as=2/(1/MAF+1) in diploid chromosomes because the MAF and ctDNA fraction are related: MAF=(ctDNA×1)/[(1−ctDNA)×2+ctDNA×1]. ctDNA detectable was defined as a ctDNA fraction > 0%.
4. The measurement of time to disease recurrence and the comparison of alteration frequency
The study endpoint was postoperative BCR. BCR was defined according to the European Association of Urology (EAU) Guidelines on Prostate Cancer (2017 edition): following RP, BCR is defined by two consecutive rising PSA values > 0.2 ng/mL [4]. Biochemical progression-free survival (bPFS) was defined as the time from initial RP to BCR. To evaluate the differences in genomics across nmPCa to meta-static PCa (mPCa), we compared the alteration frequency among the studied patients with ctDNA fraction > 2.0% with our previously published mPCa cohort [20].
5. Statistical analysis
All statistical analyses were completed using R ver. 3.6.0 (R Foundation for Statistical Computing, Vienna, Austria). Clinical characteristics were summarized by different cohorts using descriptive statistics. The Kaplan-Meier method was used to estimate the bPFS of different groups of patients, and differences between groups were analyzed using the log-rank test in the survival package (v.2.44.1.1). Univariate and multivariate Cox regression analysis were used to calculate the hazard ratios (HR) and 95% confidence intervals (CIs). Only factors significant in univariate analysis were included in the subsequent multivariate analysis.
Results
1. Patients’ clinicopathological features
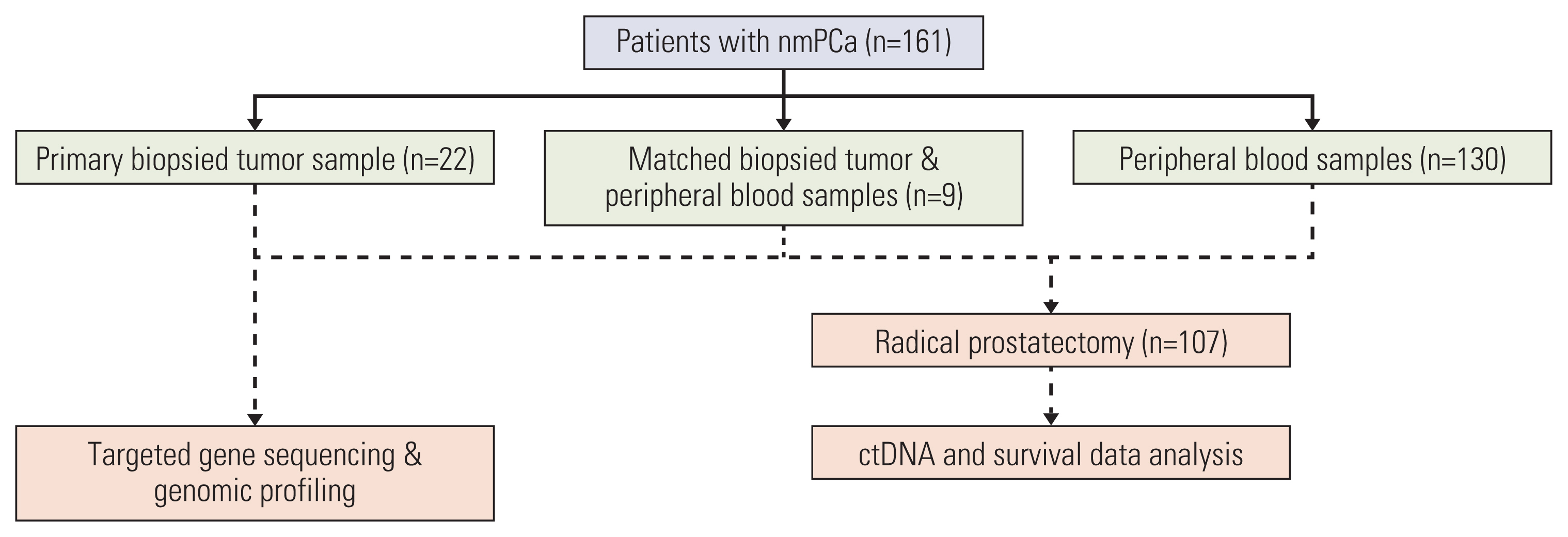
We conducted a retrospective genomic analysis on prospectively collected peripheral blood samples and biopsied tumor tissue samples from 161 patients with nmPCa involved in the present study. The schema of the study was presented in Fig. 1. At the time of writing, 107 of the 139 ctDNA sequenced patients received RP at the Ren Ji Hospital, of which 73 with high-risk PCa had received neoadjuvant hormonal therapy involving upfront subcutaneous injection of leuprorelin/goserelin and oral bicalutamide for a 3-month period. The remaining 32 of the 139 ctDNA sequenced patients were pragmatically addressed to active surveillance, hormonal therapy, or radiotherapy based on clinicians’ judgment, which were excluded from the post-prostatectomy survival analysis. The clinicopathological features of the studied patients with ctDNA analysis were summarized in Table 1.
2. The genomic profiles of the studied patients
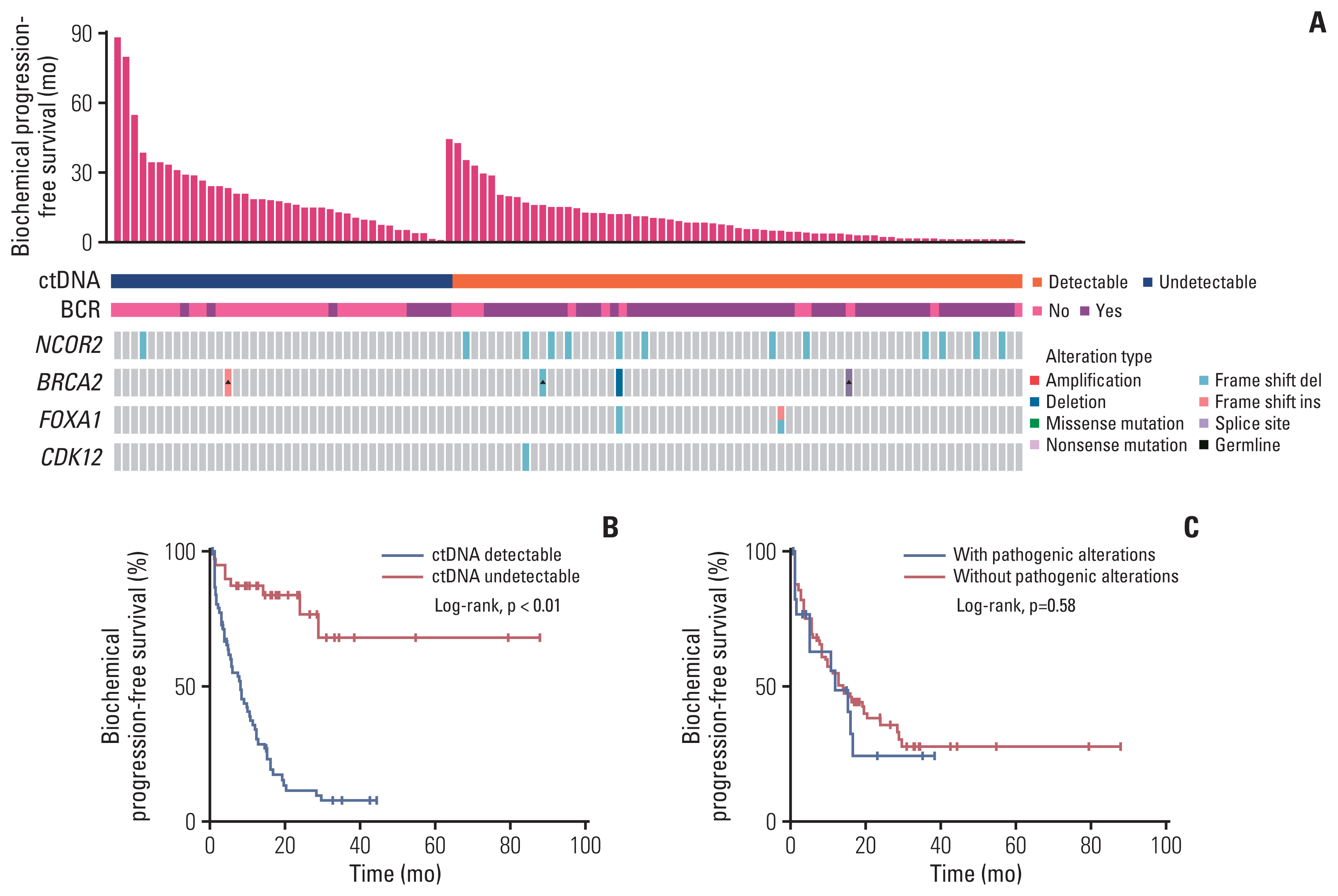
We successfully sequenced 139 ctDNA samples and 31 biopsied tumor tissue samples, among which nine patients had ctDNA and concurrent biopsied tumor tissue samples available. The genomic landscape of all the studied patients was shown in Fig. 2A. Among the patients with ctDNA samples, 91 (65.5%) had detectable ctDNA and 61 (43.9%) had ctDNA fraction > 2.0%. In the population as a whole, NCOR2 (11.8%, n=19) was the most frequently altered gene, followed by BRCA2 (3.7%, n=6), ATR (2.5%, n=4), and CDK12 (2.5%, n=4). Among the nine patients with matched samples, except that three patients had undetectable ctDNA and did not have any deleterious alteration in tumor tissue samples, no shared alteration was found in ctDNA samples and tumor tissue samples of the remaining six patients (Fig. 2B). We compared the genomic landscape of deleterious alterations of our nmPCa cohort (n=161) to that of The Cancer Genome Atlas (TCGA) primary cancer cohort (n=333) [21]. As shown in S1 Fig., the alteration frequencies of ATM and TP53 were significantly lower in our nmPCa cohort compared to the TCGA cohort (ATM, 0.62% vs. 3.90%, p=0.043; TP53, 1.86% vs. 6.91%, p=0.018), while other commonly altered genes showed similar frequencies.
3. The comparison of alteration frequencies between patients with nmPCa and mPCa
To further evaluate the genomic features in nmPCa, we generated the data set that contains genomic profiles of patients with ctDNA fraction > 2.0% across three distinct clinical states including nmPCa, metastatic castration-sensitive PCa (mCSPC), and metastatic castration-resistant PCa (mCRPC). Remarkably, we noticed that patients with nmPCa displayed lower mutation burden, whereas those with mPCa displayed much higher (Fig. 2C). RB1 alteration was absent in the nmPCa cohort compared with 7.3% in mCSPC cohort and 7.9% in mCRPC cohort. AR alteration was obviously enriched in mCRPC cohort. The other genes including FOXA1, SPOP, BRCA2, CDK12, TP53, and PTEN were more frequently altered in both mCSPC cohort and mCRPC cohort.
4. The association between the clinicopathological features and ctDNA status
The overview of the clinicopathological features of the studied patients according to ctDNA status was shown in S2A Fig. The proportion of detectable ctDNA samples seemed to be higher among the patients with high Gleason score compared with those with low Gleason score (70.5% vs. 58.3%, p=0.153). Patients at clinical T3–4 category or N1 category tended to have a higher ctDNA detection rate compared with those at clinical T1–2 category (65.9% vs. 62.4%, p=0.846) or N0 category (71.9% vs. 61.8%, p=0.399). The proportion of detectable ctDNA was lower among the patients with low PSA level (S2B Fig.).
5. ctDNA status before treatment is associated with increased risk of BCR
Overall, 107 patients had received RP and their recurrence-free survival data according to ctDNA status were illustrated in Fig. 3A. Only eight of 39 patients (20.5%) with undetectable ctDNA had achieved BCR at the time of writing, whereas 56 of 68 patients (85.3%) with detectable ctDNA had achieved BCR. Patients who had undetectable ctDNA experienced significantly longer bPFS compared with those who had detectable ctDNA (not available [NA] vs. 8.2 mo; HR, 0.14; 95% CI, 0.09 to 0.24; p < 0.01) (Fig. 3B). Additionally, patients with or without pathogenic alterations had similar risk of BCR (12.0 vs. 14.1 months, p=0.579) (Fig. 3C).
6. The prognostic value of ctDNA status remains significant across subgroups
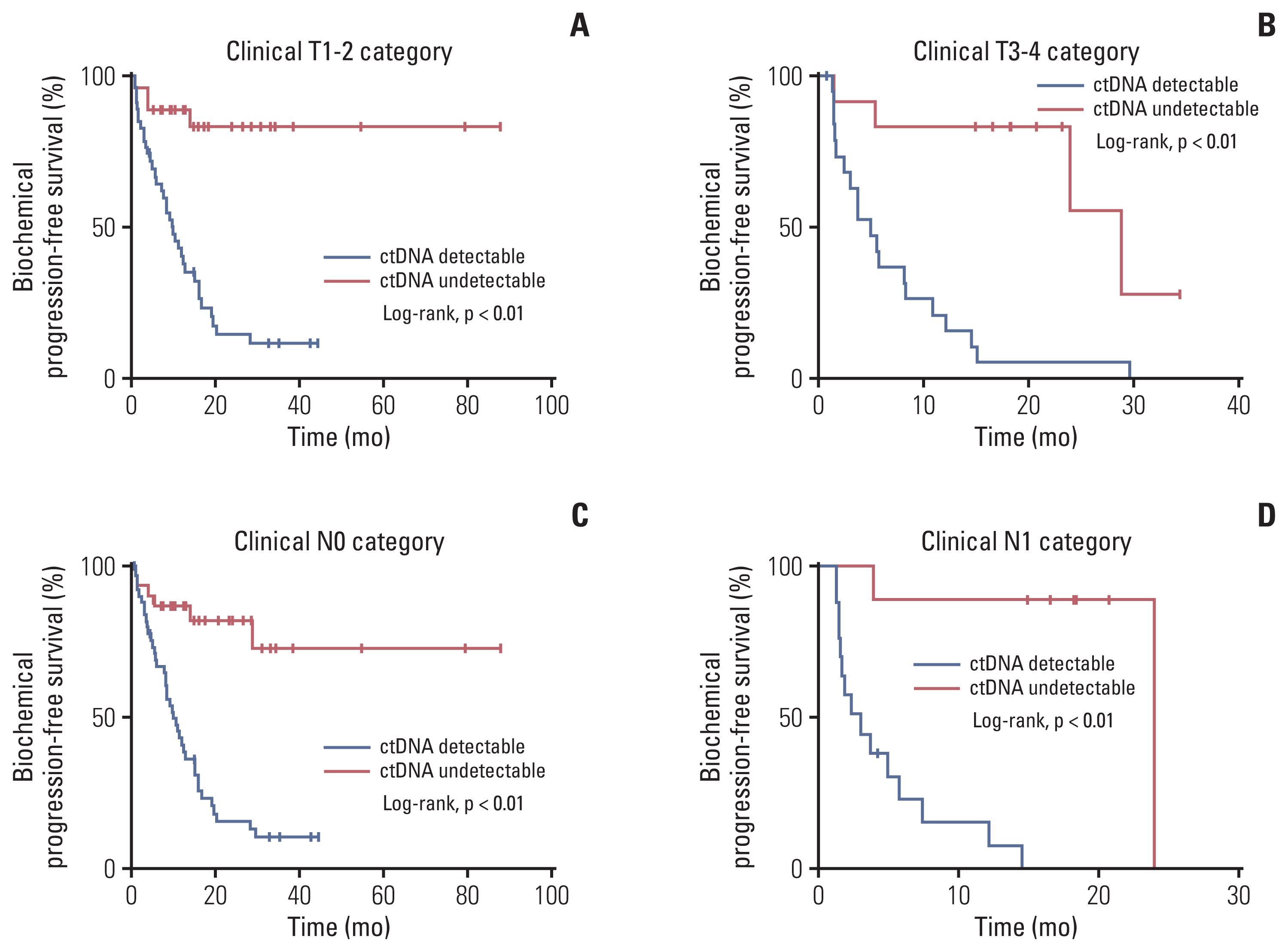
In the cohort at clinical T1–2 category, only 4 of 27 patients (14.8%) with undetectable ctDNA had experienced BCR and 36 of 47 patients (76.6%) with detectable ctDNA had relapsed at a median follow-up of 10.0 months (NA vs. 10.0 mo; HR, 0.13; 95% CI, 0.07 to 0.24; p < 0.01) (Fig. 4A). In patients at clinical T3–4 category who had detectable ctDNA, the median bPFS was 4.9 months. In the cohort with undetectable ctDNA, the median bPFS was 28.8 months (HR, 5.7; 95% CI, 2.5 to 13.0; p < 0.01) (Fig. 4B). Similar findings were noted in the cohorts at clinical N0 and N1 category. In the cohort at clinical N0 category, only six of 30 patients (20.0%) with undetectable ctDNA had experienced BCR and 40 of 50 patients (80.0%) with detectable ctDNA had relapsed at a median follow-up of 10.0 months (NA vs. 10.0 months; HR, 0.17; 95% CI, 0.09 to 0.29; p < 0.01) (Fig. 4C). In patients at clinical N1 stage who had detectable ctDNA, the median bPFS was 3.0 months. In the cohort with undetectable ctDNA, the median bPFS was 24.0 months (Fig. 4D). Univariate analysis of six variables was carried out in Table 2. Pre-operative ctDNA fraction as a continuous variate was not a statistically significant predictor (HR, 6.223; 95% CI, 0.842 to 45.967; p=0.073), while ctDNA status (undetectable vs. detectable) was significantly associated with the bPFS (HR, 0.136; 95% CI, 0.064 to 0.287; p < 0.001). HRs for other variables all trended in the expected direction but did not reach statistical significance.
Discussion
This is the first biomarker study that assessed the prognostic value of pre-operative ctDNA in predicting the disease recurrence of patients with nmPCa undergoing radical procedure. Our results revealed the genomic profiles of the patients with nmPCa and found low detection rate of deleterious alterations. Despite the limitations of ctDNA detection in a localized setting, we demonstrated the clinical utility of ctDNA as a reliable tool to reflect the overall mutational status, allowing for monitoring disease progression.
Although the target gene sequencing via liquid biopsy for nmPCa is hampered by the low overall abundance of ctDNA [22], we found that ctDNA was detectable 65.5% of the studied patients, which is consistent with a previous study that has reported the variant detection rate of 57% [23]. Additionally, the clinicopathological features including PSA, Gleason score, and clinical stage were not strongly associated with the ctDNA status in the present study, but the patients with aggressive disease subtypes tended to have detectable ctDNA. Our data might suggest the use of ctDNA analysis in the patients with more aggressive PCa at the time of diagnosis. Specially, we observed that ctDNA samples shared no concurrent alteration with tumor samples. As ctDNA proves to have the potential ability to capture both likely clonal and subclonal alterations from multiple tumor cell populations [23], our results substantially support that ctDNA reflecting the comprehensive mutational status could be used in the evaluation of heterogeneous nmPCa.
The landscape of deleterious alterations of our nmPCa cohort was overall similar to that of the TCGA primary PCa cohort. However, the frequencies of ATM and TP53 were significantly lower in our cohort. Ethnic differences may contribute to these results, as over 80% of the TCGA cohort are Caucasians while our cohort consists of Chinese patients [21]. In line with our results, a report of genomic and epigenomic analyses in 208 Chinese primary PCa patients revealed a relatively lower frequency of TP53 and ATM copy number variations compared to Western cohorts [24]. To better understand the genetic landscape in Chinese men with PCa, we compared the distribution of genomic alterations between the nmPCa cohort and the mPCa cohort from our previous study [20]. Interestingly, the genomic profiles of the patients with nmPCa revealed low detection rate of somatic deleterious alterations. In the localized setting, the genes involved in androgen receptor pathway, DNA damage repair pathway, and cell cycle pathway were less frequently altered compared with the mPCa cohort. This is possibly because of the low disease burden and low abundance of DNA shed by tumor, underscoring the distinct genomic basis of indolent and non-indolent disease. Serial studies have demonstrated that numerous genomic alterations in ATM, FOXA1, and PTEN were predictive of disease phenotype and progression [24–26]. However, the predictive power of ctDNA for the disease recurrence in nmPCa setting remains unclear.
A previous study highlighted that the TP53 ctDNA status was strongly associated with BCR and metastasis [27]. Similarly, our preliminary results suggest a potential role of pre-operative ctDNA as a predictive biomarker for disease recurrence. In the present study, 85.3% of patients with detectable ctDNA have experienced BCR at a median follow-up of 8.2 months after RP regardless of the neoadjuvant treatment. This might suggest that pre-operative ctDNA is enough informative to filter out the population at an increased relapse risk where immediate postoperative therapy should be considered and individualized neoadjuvant therapy could be explored. Consistent with multiple ctDNA studies in the localized setting [10,11,15–17], our data support that ctDNA could detect the existence of micro-metastasis and minimal tumor-derived molecules. In the era of precision medicine, our study provides new insights into the clinical utility of ctDNA in nmPCa that would open new frontiers and perspectives for disease monitoring and individualized interventions.
The present study has several limitations including its retrospective nature and the absence of study design and validation cohort. In addition, we were unable to control the clinical features in a real-world setting. A subgroup of nmPCa patients with sequencing data was addressed to treatment regimens other than surgery, which may cause potential selection bias in our survival analysis. Lastly, the postoperative ctDNA was not collected, since the serial changes in ctDNA were of great importance in reflecting treatment response [28,29]. We confirm that prospective ctDNA studies in the setting of resectable PCa would be conducted in a larger population in the near future.
To our knowledge, our study is one of the first studies to highlight the prognostic value of ctDNA in the nmPCa setting. Pre-operative ctDNA detection could identify the patients at high risk of recurrence and has the clinical potential to inform immediate postoperative interventions, but these approaches remain to be validated in prospective studies. It is of great importance that ctDNA studies provide insights into accurate monitoring and precise treatment rather than simply following routine clinical care.
In this study, we present a preliminary genomic atlas of nmPCa via liquid biopsy, which reveals the predictive power of pre-operative ctDNA for disease recurrence. Comparative analysis demonstrated low detection rate of somatic deleterious alterations in the nmPCa setting. Importantly, ctDNA reflecting the comprehensive mutational status could identify the patients at high risk of recurrence and has the clinical potential to inform immediate postoperative interventions, which provides insights into accurate monitoring and precise treatment.