INTRODUCTION
Since the mid-1970s, the Durie/Salmon (DS) system has been the most widely used staging system for multiple myeloma (1). It uses several variables, including hemoglobin, calcium, monoclonal protein, the number of bone lesions and creatinine. Although the DS system has been proven to be an effective staging tool for patients with multiple myeloma, several problems have developed with the use of this staging system such as the complexity and difficulty in evaluating the lytic bone lesions as this evaluation is observer dependent. Thus, a more reliable staging system is needed.
Two new staging systems, the Southwest Oncology Group (SWOG) staging system and the International Staging System (ISS) have recently been developed (2,3). Both the SWOG and ISS staging systems are based on the serum β2-microglobulin and serum albumin levels, which are two important prognostic factors for multiple myeloma patients. The difference between these two systems is that the ISS consists of 3 stages whereas the SWOG staging system consists of 4 stages.
There is little data on the SWOG staging system and the ISS in Korea. Therefore, to investigate the validity of these two new staging systems for predicting survival, we compared the DS staging system, the SWOG staging system and the ISS in Korean patients with multiple myeloma.
MATERIALS AND METHODS
Between 1992 and 2005, we enrolled a total of 85 consecutive patients who were diagnosed with multiple myeloma at Hanyang University Hospital and their baseline values of albumin and β2-microglobulin were available. Forty-one (48.2%) were men and 44 (51.8%) were women and their median age was 63 years (range: 36~87). The clinical and laboratory data were retrospectively obtained. The collected data included their age at diagnosis, gender, the type and amount of M protein, hemoglobin, the platelet count, the serum calcium, LDH, creatinine, albumin and β2-microglobulin, the number of lytic bone lesions and the percentage of bone marrow plasma cells. The institutional review board of Hanyang University Guri Hospital approved this study.
For comparison of the three staging systems, the patients were initially classified as DS stage I, II and III. The same patients were then restaged using the SWOG staging system and the ISS, according to their serum β2-microglobulin and serum albumin levels at the time of diagnosis. The SWOG staging system and the ISS are shown in Table 1.
Overall survival was measured from the date of diagnosis to the date of death or the last follow-up. Survival curves were estimated using the Kaplan-Meier method and they were compared with the log-rank test. Stepwise Cox's regression analysis was performed to identify the prognostic factors for survival. For all tests, p<0.05 was considered statistically significant.
RESULTS
1) Patient characteristics
The most common type of multiple myeloma was IgG (52.9%), followed by IgA (22.4%), light chain (21.2%), IgD (2.4%), and one case of the non-secretory type. The median percentage of plasma cells in the bone marrow of the patients was 40%. Nineteen patients received high dose therapy with autologous stem cell transplantation and 65 patients were treated with conventional chemotherapy such as melphalan and prednisone, the M2 protocol (cyclophosphamide, vincristine, BCNU, melphalan and prednisone), or VAD (vincristine, adriamycin and dexamethasone). The number of deaths was forty-nine (57.6%). The most common cause of death was disease progression (40 patients), while other causes of death included infection (7 patients), acute myocardiac infarction (1 patient) and hepatoma (1 patient). The median follow-up duration was 64.4 months and the median overall survival for all patients was 25.4 months.
2) Survival according to the 3 staging systems
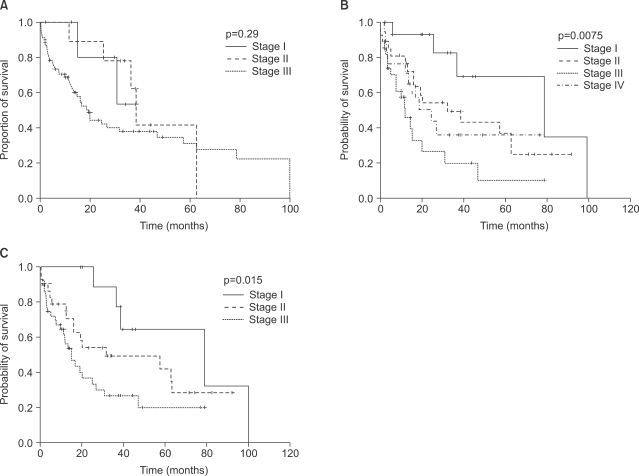
When staged by the DS system, 10 patients were stage I (11.8%), 6 patients were stage II (7.1%) and 69 patients were stage III (81.2%). The median survivals of each DS stage were 38.6 months for stage I, not reached for stage II (the median follow-up duration of the stage II patients was 32.5 months), and 19.4 months for stage III (p=0.29, Fig. 1A). The DS staging system was not able to predict survival. For the SWOG staging system, 14 patients were stage I (16.4%), 27 patients were stage II (31.8%), 27 patients were stage III (31.8%) and 17 patients were stage IV (20.0%). The median survivals of the SWOG staging system for stages I, II, III and IV were 78.6 months, 31.8 months, 11.6 months and 24.8 months, respectively (p=0.0075, Fig. 1B). The median survival for stage IV was longer than that for stage III. For the ISS, 11 patients were stage I (12.9%), 30 patients were stage II (35.3%) and 44 patients were stage III (51.8%). The median survivals of the ISS stages I, II and III were 78.6, 31.8 and 15.1 months, respectively (p=0.015, Fig. 1C). The ISS provided the best prediction of overall survival for multiple myeloma patients.
3) Prognostic factors
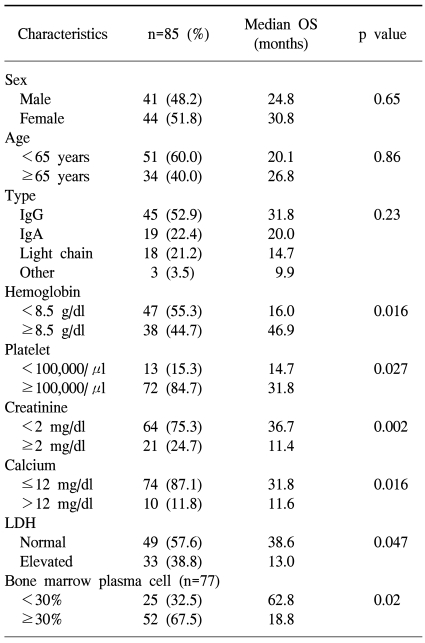
Other variables associated with significantly shorter survival according to the univariate analysis included a hemoglobin level <8.5 g/dL (p=0.016), a platelet count<100,000/µl (p=0.027), a creatinine level ≥2 mg/dl (p=0.002), a calcium level >12 mg/dl (p=0.016), a bone marrow plasma cell count ≥30% (p=0.02) and an elevated LDH level (p=0.047, Table 2). Multivariate analysis revealed that none of these were independent significant prognostic factors for improved overall survival.
DISCUSSION
Because of the various outcomes of patients with multiple myeloma, determining the prognostic factors of multiple myeloma is important for predicting disease outcome and determining the treatment method. Until now, a number of prognostic factors have been identified including hemoglobin, calcium, creatinine, β2-microglobulin (4,5), albumin (6), C-reactive protein (7), the plasma cell labeling index (8) and chromosomal 13 deletion or other chromosomal abnormalities (9). Among these, β2-microglobulin has been the single most important prognostic factor for predicting survival and it is correlated with the tumor burden and renal function (6). The serum albumin may reflect the interleukin-6 levels, the liver function and the nutritional status (2).
The ISS was developed based on data analysis of 10,750 previously untreated myeloma patients from 15 Asian, European and North American institutions and groups (3). β2-microglobulin and albumin were selected because they were statistically powerful prognostic factors and these required only simple inexpensive tests. The median survivals of ISS stage I, II and III were 62, 44, and 29 months, respectively (p<0.0001). In addition, the ISS was demonstrated to be an effective system regardless of the geographic region, age and treatment type (3).
It was recently published that the SWOG and the ISS systems at the time of diagnosis could predict the prognosis of multiple myeloma patients who have undergone high dose chemotherapy with autologous peripheral stem cell transplantation as a first-line therapy (10). Furthermore, it was also published that the overall survival could be predicted by the SWOG system (p=0.02) and the ISS (p=0.01), but not by the DS staging system (p=0.25). One study that evaluated the significance of five staging systems in 470 multiple myeloma patients showed the superiority of the ISS over the DS staging system and the other prognostic classifications based on a combination of β2-microglobulin and albumin (11).
Our study showed similar results. The DS system could not show a significant survival difference between stages I, II, and III. Using the ISS and SWOG staging system at diagnosis, the overall survival was significantly different among the multiple myeloma patients of each stage.
However, in our study, the median survival of stage IV patients in the SWOG staging system was longer than that for the stage III patient. Another study by Kim (10) also showed similar results in that the median survival of stage IV (45.5 months) was longer than that of stage III (37.1 months). Yet another previous study (11) revealed that the overall survival was similar between patients in SWOG stage III (23 months) and IV (21 months). The difference between SWOG stages III and IV was the serum albumin level, and although these studies included a relatively small number of patients, these results suggest that the prognostic value of albumin might be weak for patients with high β2-microglobulin levels. So, the ISS may be a more reliable and predictable system than the DS and the SWOG staging systems.
Our study has several limitations. First, the treatment methods of the patients were heterogeneous. Second, the clinical data was analyzed retrospectively. Third, a relatively small number of patients were examined in this study. Nevertheless, our results suggested that the ISS might be a more useful, reliable and simple staging system for multiple myeloma patients than either the SWOG or DS staging systems.