Changes in Invasive Breast Carcinomas after Neoadjuvant Chemotherapy Can Influence Adjuvant Therapeutic Decisions
Article information

Abstract
Purpose
Neoadjuvant chemotherapy (NACT) can change invasive breast carcinomas (IBC) and influence the patients’ overall survival time (OS). We aimed to identify IBC changes after NACT and their association with OS.
Materials and Methods
IBC data in pre- and post-NACT samples of 86 patients were evaluated and associated with OS.
Results
Post-NACT tumors changed nuclear pleomorphism score (p=0.025); mitotic count (p=0.002); % of tumor-infiltrating inflammatory cells (p=0.016); presence of in situ carcinoma (p=0.001) and lymphovascular invasion (LVI; p=0.002); expression of estrogen (p=0.003), progesterone receptors (PR; p=0.019), and Ki67 (p=0.003). Immunohistochemical (IHC) profile changed in 26 tumors (30.2%, p=0.050). Higher risk of death was significatively associated with initial tumor histological grade III (hazard ratio [HR], 2.94), high nuclear pleomorphism (HR, 2.53), high Ki67 index (HR, 2.47), post-NACT presence of LVI (HR, 1.90), luminal B–like profile (HR, 2.58), pre- (HR, 2.26) and post-NACT intermediate mitotic count (HR, 2.12), pre- (HR, 4.45) and post-NACT triple-negative IHC profile (HR, 4.52). On the other hand, lower risk of death was significative associated with pre- (HR, 0.35) and post-NACT (HR, 0.39) estrogen receptor–positive, and pre- (HR, 0.37) and post-NACT (HR, 0.57) PR-positive. Changes in IHC profile were associated with longer OS (p=0.050). In multivariate analysis, pre-NACT grade III tumors and pre-NACT and post-NACT triple negative IHC profile proved to be independent factors for shorter OS.
Conclusion
NACT can change tumor characteristics and biomarkers and impact on OS; therefore, they should be reassessed on residual samples to improve therapeutic decisions.
Introduction
Invasive breast carcinomas (IBC) treatment involves local control (surgery and radiotherapy), usually associated with systemic therapies, guided by tumor stage, histological characteristics and tumor biomarkers status, including hormone receptors (estrogen receptor [ER] and progesterone receptor [PR]), human epidermal growth factor receptor 2 (HER2) and Ki67 status, which are assessed in all new breast cancer cases by immunohistochemical staining (IHC). These prognostic and predictive factors give information about clinical outcome and predict response to specific therapies, thus influence the best individual treatment decision [1-3].
Systemic therapies can be administered before (neoadjuvant) and/or after surgical resection (adjuvant). Neoadjuvant chemotherapy (NACT) is used as the initial treatment for patients with inoperable tumors, for operable tumors to downstage and allow more conservative surgical excisions (both in the breast and in the axilla), for early-stage tumors (especially triple-negative and HER2-positive), and in highly proliferative tumors, as they show better response to systemic therapy [1-5]. Information about response to neoadjuvant therapy response also allows adjuvant therapy decision. NACT can result in pathological complete response (pCR), partial response with residual disease, and tumor progression [3,5]. An important tool developed by a group in the MD Anderson Cancer Center is the Residual Cancer Burden (RCB) calculator, which includes pathological parameters of the residual tumor, and is related with tumor progression and patients’ overall survival [6].
In cases with residual disease after NACT, tumor morphological characteristics and IHC status may be discordant with those in the initial biopsy sample, due to several factors, like intratumoral heterogeneity (genetic alterations during the clonal evolution of the tumor cells resulting in subclones with different responses to therapy) and sampling variability [1,7,8]. In metastatic IBC, the American Society of Clinical Oncology and College of American Pathologists (ASCO/CAP) guidelines recommend re-biopsy of breast cancer metastases to re-evaluate ER, PR, and HER2 status [9]. Although several authors have reported pathological changes in residual tumors, there is still no consensus if biomarkers should be retested in post-NACT samples and if these changes should be considered in the adjuvant setting [1-4,7,8,10].
This study aims to evaluate the effects of NACT on IBCs and identify their influence on patient’s overall survival time, in a single Public Health Institution in Brazil.
Materials and Methods
1. Study group and histological review
From the archives of the Mammary Pathology Laboratory of the Faculty of Medicine – Federal University of Minas Gerais (UFMG), 86 patients with IBC treated at the Hospital of Clinics between 2008-2018, who underwent NACT prior to surgical resection were retrospectively selected. All cases with clinicopathological data and both pre- and post-therapy formalin-fixed paraffin-embedded (FFPE) samples available were included. pCR was defined as the absence of residual invasive disease in the breast and lymph nodes [10].
Clinical data were collected via review of the archives and medical records to evaluate disease stage and overall survival time of patients. Patients received NACT according to standard protocols of Brazilian’s unified public health system (Sistema Único de Saúde, SUS) [11].
All pathological data were reviewed by a breast pathologist (C.B.N.), as tumor histologic type and grade, percentage of tumor infiltrating inflammatory cells, presence of lymphovascular invasion (LVI), presence of associated in situ carcinoma, and IHC tests for ER, PR, HER2, and Ki67 were repeated in our lab.
Tumors were classified according to the World Health Organization diagnostic criteria [12]. For statistical analysis, the histological tumor types were divided in three groups: invasive carcinoma of no special type (Ductal NST), invasive lobular carcinoma, and IBCs of other specific types. Histological grade was evaluated in accordance with the Nottingham (modified Scarff-Bloom-Richardson) system [13]. Tumor infiltrating inflammatory cells were divided in three levels, based on their percentage compared to the tumor cells: absent (less than 1%), low (1 to 20%), and high (over 21%). Tumors were staged according to the American Joint Committee on Cancer 8th edition (anatomic stage) [14].
The RCB was calculated based on primary tumor bed area, percentage of overall residual cancer cellularity, percentage of in situ carcinoma, number of positive lymph nodes and diameter of largest metastasis. The RCB calculator is free and available at http://www3.mdanderson.org/app/medcalc/index.cfm?pagename=jsconvert3 [6].
2. IHC assays and evaluation
The FFPE of pre- and post-therapy blocks were submitted to microtomy, obtaining 4 μm histological sections placed on electric charged slides, submitted to the IHC technique using ready-to-use antibodies from Agilent Technologies, and the antigen reactivation was performed by water bath or steamer. The clones used were as follows: for ER, 1D5 – PharmaDX (Dako Cytomation, Glostrup, Denmark), for PR, PGR1294 – PharmaDX, for HER2, A0485 – HercepTest (Dako, Carpinteria, CA), and for Ki67, MIB1.
All tests were performed at the Mammary Pathology Laboratory of the Medical Faculty of UFMG, using standardized protocols according to the manufacturers’ recommendations. Known positive and negative controls were included.
The interpretation of the results followed the latest ASCO/CAP guidelines for ER, PR, and HER2 protein expression [15,16]. A positive ER and PR tumor showed more or equal of 1% of cells staining and results were semi quantitative with percentage and intensity of positive cells (Allred score). The HER2 3+ cases were considered positive, 2+ cases were considered equivocal and sent for HER2 gene amplification test by fluorescence in situ hybridization (FISH) analysis in an external service to determine HER2 status (which was interpreted as HER2 positive if the ratio HER2/chromosome enumeration probe 17 was ≥ 2.0 and the average HER2 copy number was ≥ 4.0 signals/cell or negative otherwise), and 0 or 1+ were considered negative [16]. Ki67 expression analysis was semi-quantitative, with the average percentage of tumor-stained nuclei, in at least 300 tumor cells. The median was calculated using the percentage of Ki67 expression of all cases, and the cut-off point was defined for low (< 28%) or high (> 28%) Ki67 index [17].
According to the biomarker’s expression, the tumors were divided into four groups: luminal A–like: positive ER and PR, negative HER2 and low Ki67; luminal B–like: positive ER, any expression of PR, with positive HER2 and any expression of Ki67 or negative HER2 with high Ki67; HER2-positive: negative ER and PR, positive HER2 and any expression of Ki67; and triple-negative: negative ER, PR, and HER2 with any expression of Ki67 [18].
3. Statistical analysis
Statistical analysis was performed using the SPSS statistical program ver. 29 (IBM Corp., Armonk, NY). To compare pre- and post-therapy variables, the McNemar test was used for dichotomous variables and the McNemar-Bowker for variables with more categories. The Wilcoxon’s test was used to analyze pre- and post-therapy continuous variables.
Factors associated with overall survival time of patients were analyzed using Kaplan-Meier curves and compared with the log-rank test. The Cox proportional hazards model was also used. Hazard ratios (HR) and 95% confidence intervals (CI) were calculated. Two multivariate models were constructed: one based on pre and the other on postNACT characteristics. A backward-conditional strategy was used. The tests were considered statistically significant when p-value was < 0.05.
Results
1. Clinicopathological characteristics
The clinical characteristics, NACT regimen and their association with overall survival (univariate analysis) are summarized in Table 1. Patient’s age at diagnosis ranged from 24 to 75 years old (mean±standard deviation, 49.65±10.96 years). The patient’s age at the time of diagnosis influenced overall survival, with a lower risk of death with each additional year of age (HR, 0.98; 95% CI, 0.96 to 1.00; p=0.046).
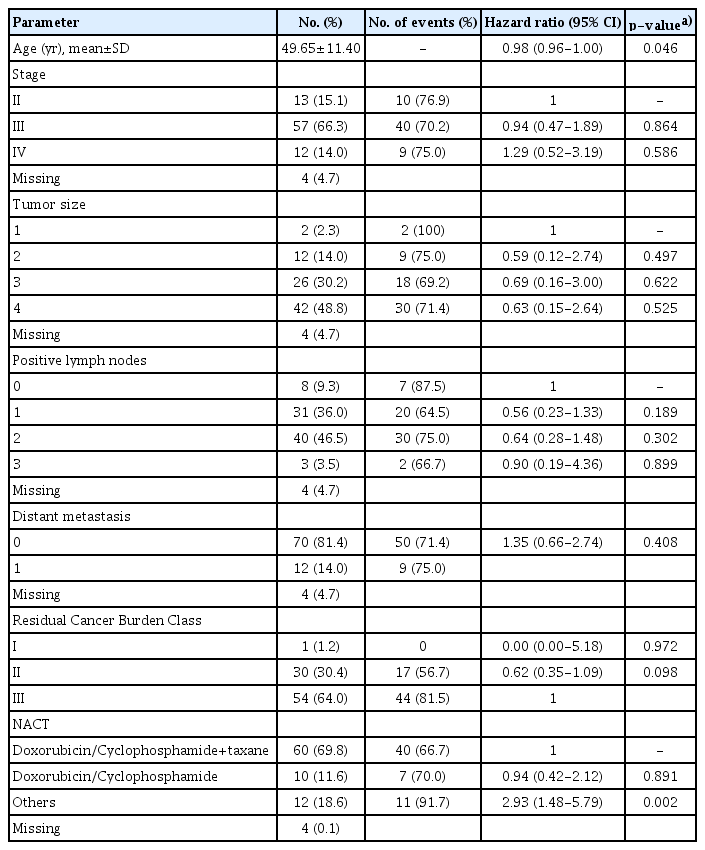
Clinical characteristics, survival analysis, and treatment regimen of 86 invasive breast carcinomas (univariate analysis)
Pre-NACT tumor samples were core needle biopsies (51 cases, 59.3%) and incisional biopsies (35 cases, 40.7%); post-NACT tumor samples were from mastectomies (70 cases, 81.4%) and breast conserving surgeries (16 cases, 18.6%).
Information regarding chemotherapy regimens was available for 82 patients (95.3%) (Table 1). The most common neoadjuvant regimen was doxorubicin plus cyclophosphamide followed by a taxane (60 patients, 69.8%). Four out of 48 pre-NACT ER-positive cases (8.3%) also received tamoxifen before surgery. In this study, only three out of 11 (27.3%) HER2-positive patients received neoadjuvant trastuzumab. In the adjuvant setting, all 37 patients with post-NACT ER-positive tumors and 11 patients whose tumors changed to ER-negative after NACT received tamoxifen. Six patients out of ten post-NACT HER2-positive cases (60%) received adjuvant trastuzumab.
Survival data was available from 85 patients, with a median follow-up time of 43 months (range, 8 to 161 months). Sixty-one patients (70.9%) died during follow-up.
Most patients had locally advanced or metastatic breast cancer with 57 cases (66.3%) on clinical stage III, and no cases on stage I. Four cases (4.7%) were not staged due to missing information. Tumor size cT3 or cT4 were most prevalent (68 cases, 79%), 74 (86%) had clinically positive lymph nodes and 12 (14%) had metastatic disease.
After calculating the RCB class we found: 55 cases (64%) with RCB=III, 30 cases (34.9%) with RCB=II and only one case (1.2%) with RCB=I. When associating patients’ survival with the RCB class, cases classified as RCB II had a non-significant lower risk of death when compared to RCB III cases (HR, 0.62; 95% CI, 0.15 to 1.09; p=0.098) in univariate analysis.
The pathological characteristics and their association with overall survival (univariate analysis) are summarized in Table 2, changes after NACT are in Table 3 and survival curves are shown in Fig. 1. The most prevalent initial histological characteristics were invasive carcinoma of no special type (63 cases; 73.3%), histological grade III (42 cases, 48.8%) and low tumor infiltrating inflammatory cells (55 cases, 64.0%). After NACT, the proportion of these characteristics was: 52 cases (60.5%) had invasive carcinoma of no special type (NST), 41 cases (47.7%) had histological grade III and 49 cases (57%) had low tumor infiltrating inflammatory cells. Eight tumors (9.3%) showed rare residual isolated tumor cells, limiting histological type and grade analysis.
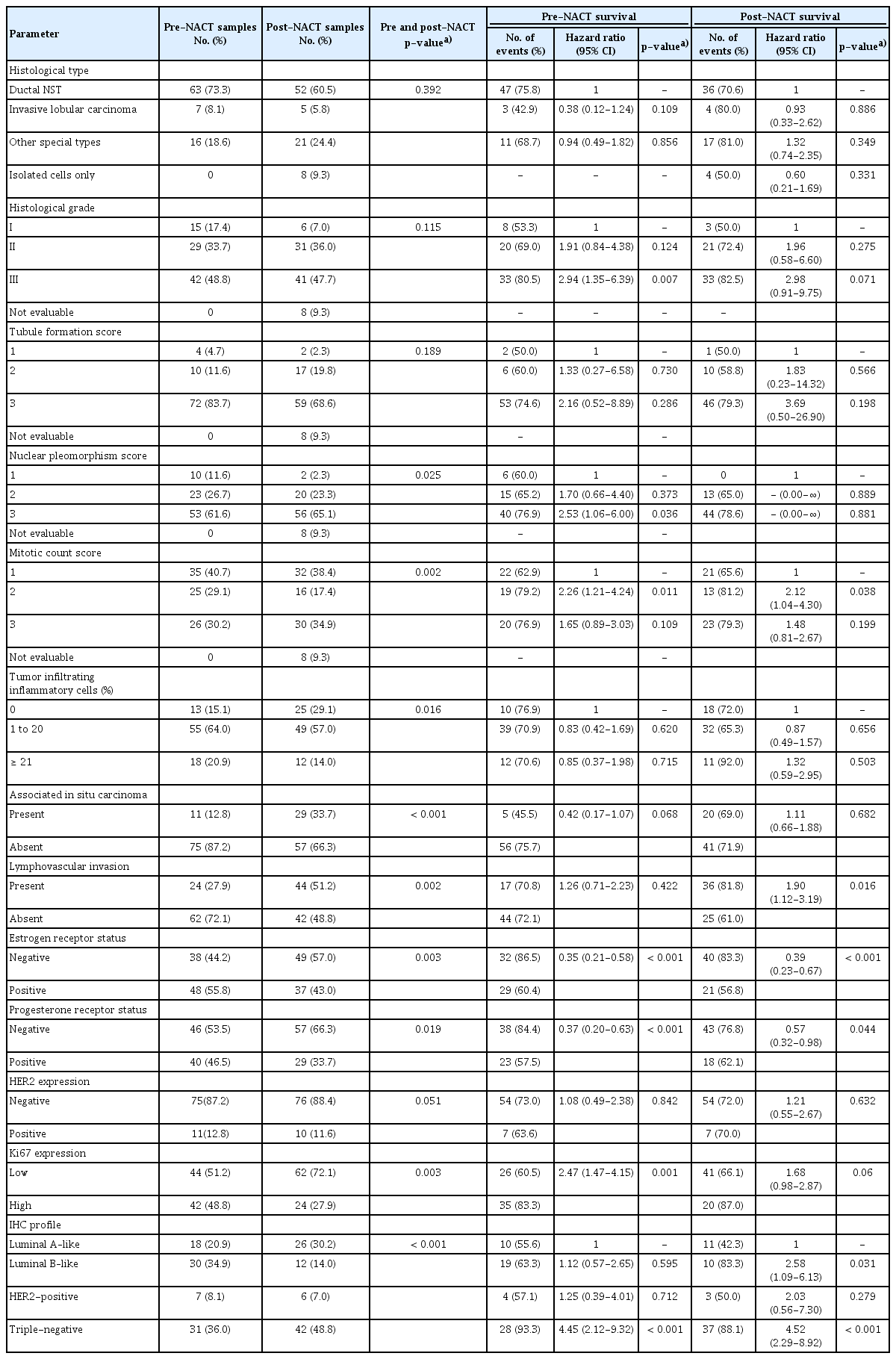
Clinicopathological characteristics of invasive breast carcinomas in pre- and post-NACT samples and univariate survival analysis

Changes on histopathological characteristics after NACT in invasive breast carcinomas samples
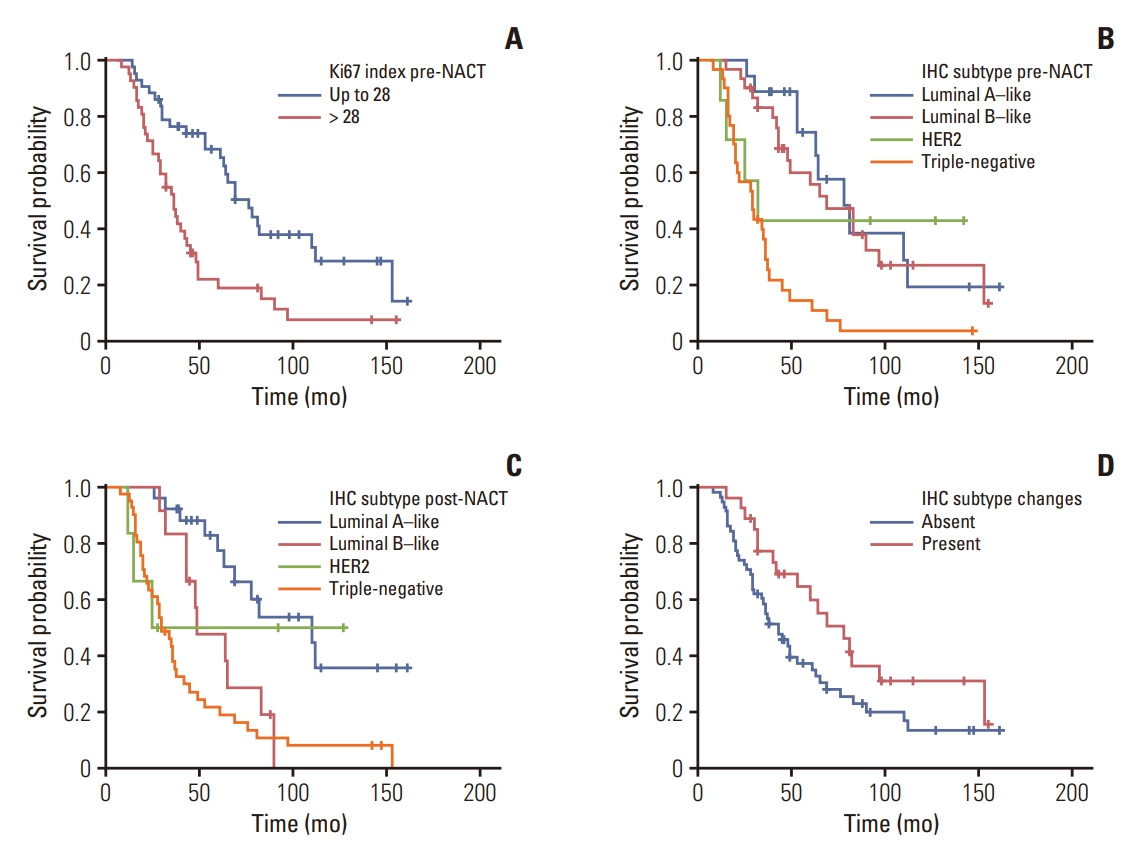
Survival probability of patients with invasive breast carcinoma according to Ki67 index in pre-NACT samples (p=0.006) (A), IHC profile in pre-NACT samples (p < 0.001) (B), IHC profile in post-NACT samples (p < 0.001) (C), and changes in IHC profiles after NACT (p=0.050) (D). HER2, human epidermal growth factor receptor 2; IHC, immunohistochemical; NACT, neoadjuvant chemotherapy.
Tumor characteristics discordance with pre- and postNACT were as follows: 19 tumors (22.1%) changed histological type (p=0.392), 10 tumors (52.7%) changed from Ductal NST to pure special types; 31 tumors (36.1%) showed changes on histological grade, 21 (24.4%) changed to a higher and 10 (11.6%) changed to a lower histological grade (p=0.115). Evaluating the three individual features for assessing histological grade, 13 tumors (16.7%) changed tubule formation score (p=0.189), 25 (32%) tumors changed nuclear pleomorphism score (p=0.025), and 37 (47.4%) tumors changed the mitotic count score (p=0.002) (Table 3).
The intratumoral infiltrating inflammatory cells changed in 43 cases (50%), showing a lower percentage in 31 (36%), and in 12 cases (14%) showing a higher percentage in the residual tumor (p=0.016).
Associated in situ carcinoma was identify more frequently in surgical speciments post-NACT, with 29 cases (33.7%) compared to 11 cases (12.8%) pre-NACT samples (p < 0.001).
LVI was identified in 24 (27.9%) initial samples, and in post-NACT samples was almost the double, with 44 cases (51.2%, p=0.002).
The following pre-NACT tumor characteristics showed association with higher risk of death in univariate analysis: histological grade 3 versus grade 1 (HR, 2.94; 95% CI, 1.35 to 6.39; p=0.007); nuclear pleomorphism grade 3 versus grade 1 (HR, 2.53; 95% CI, 1.06 to 6.00; p=0.036); and mitotic count grade 2 versus grade 1 (HR, 2.26; 95% CI, 1.21 to 4.24; p=0.011). The following post-NACT tumor characteristics showed association with higher risk of death: mitotic count grade 2 versus grade 1 (HR, 2.12; 95% CI, 1.04 to 4.30; p=0.038) and presence of LVI (HR, 1.90; 95% CI, 1.12 to 3.19; p=0.016).
2. Biomarkers’ status
The most frequent pre-NACT biomarkers expression of the initial tumors was ER-positive (48 cases, 55.8%), PR positive (46 cases, 53.5%) and HER2 negative (73 cases, 87.2%). Two cases were HER2-equivocal (2+), but one showed gene amplification by FISH and was interpretated as HER2 positive.
Triple-negative (31 cases, 36.0%) and luminal B–like (30 cases, 34.6%) were the most frequent IHC profiles, followed by luminal A–like (18 cases, 20.9%) and HER2-positive (7 cases, 8.1%).
The most frequent post-NACT biomarkers expression was ER-negative (49 cases, 57.0%), PR-negative (57 cases, 66.3%), and HER2-negative (76 cases, 88.4%). Most residual tumors had a low Ki67 rate (62 cases, 72.1%).
Except for HER2 expression, all biomarkers had significant changes after NACT, including the IHC profile.
ER status changed in 13 (15.1%) residual tumors (p=0.003), most commonly becoming negative (12 cases, 14%) (Table 3, Fig. 2A and B). Ten tumors (11.6%) showed a higher Allred ER score (% and intensity of stained cells), and 24 cases (27.9%) showed a lower ER score. The patient whose tumor turned ER from negative to positive received adjuvant hormone treatment and died within 32 months. Changes in ER status did not influence the patients’ overall survival, with a HR of 1.02 (95% CI, 0.51 to 2.03) and p=0.958.
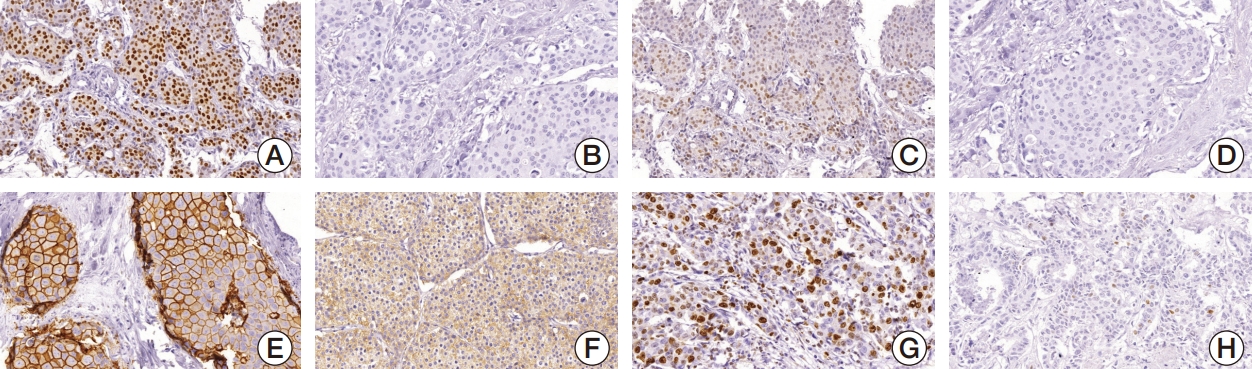
Biomarkers immunohistochemical assays (×200) of invasive breast carcinomas showing tumors: ER-positive in the pre-NACT sample (A) and negative in the post-NACT sample (B); PR positive in the pre-NACT sample (C) and negative in the post-NACT sample (D); HER2 2+ in the pre-NACT sample (E) and 0 in the post-NACT sample (F); high Ki67 index in the pre-NACT sample (G) and a low index in the post-NACT sample (H). ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; NACT, neoadjuvant chemotherapy; PR, progesterone receptor.
PR status changed in 19 (22.1%) residual tumors (p=0.019); the majority becoming negative (15 cases, 17.4%) (Fig. 2C and D). PR Allred score remained the same in 53 tumors (61.6%), seven (8.1%) changed to a higher and 26 tumors (30.2%), to a lower Allred PR score. Out of four patients who changed to PR positive, three received adjuvant hormonal therapy; 13 out of 15 patients whose tumors’ PR turned to negative didn’t use hormone therapy in the adjuvant setting, and one patient had no information about adjuvant hormone therapy. Changes in PR status did not influence the patients’ overall survival, with a HR of 0.74 (95% CI, 0.39 to 1.39; p=0.352).
HER2 expression changed from positive to negative in two tumors (p=0.051); one changed from score 2+, FISH amplified to score 0 and the other changed from score 3+ to score 1+ (Fig. 2E and F). These patients did not receive anti-HER2 neoadjuvant treatment, but one of them received anti-HER2 adjuvant treatment. HER2 scores changed in 13 tumors (15.1%, p > 0.99). Curiously, one score 3+ tumor changed to score 2+ but was FISH amplified. Changes in HER2 status did not influence the patients’ overall survival, with a HR of 0.05 (95% CI, 0.00 to 17.22; p=0.309).
Ki67 index changed in 52 tumors (60.5%), the majority to a lower index (Fig. 2G and H). Median Ki67 expression changed from 28% (95% CI, 25.6 to 32.7%) in pre-NACT to 18% (95% CI, 19.2 to 28.2) in post-NACT samples (p=0.004). The distribution of the data in relation to Ki67 expression was different when comparing pre-therapy with post-therapy tumor samples. Before NACT, the data showed a normal distribution and after NACT the data were skewed to the right (Fig. 3).
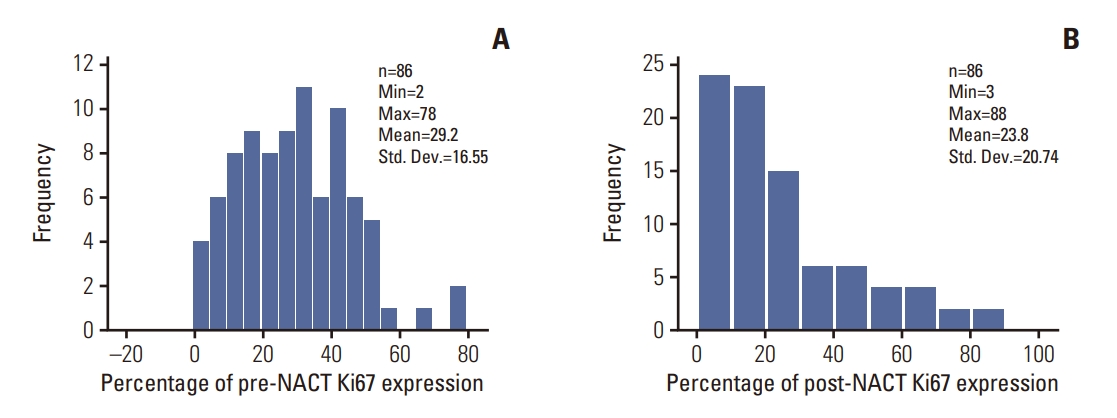
Distribution of pre- and post-NACT Ki67 index in 86 invasive breast carcinomas (p=0.004). NACT, neoadjuvant chemotherapy.
Triple-negative (42 cases, 48.8%) and luminal A–like (26 cases, 30.2%) were the most frequent IHC profiles of the residual tumors, followed by luminal B–like (12 cases, 14.0%) and HER2-like (6 cases, 7.0%). Most tumors maintained the same IHC profile (60 cases, 69.8%) (Fig. 4). Twenty-six tumors (30.2%) showed changes after NACT (p < 0.001): four tumors were initially luminal A–like, 20 were luminal B–like and 2 were HER2. Interestingly, none of the initial triple-negative and only one HER2-positive tumor changed subtype in residual tumors. Five metastatic patients changed the subtype: one from luminal B to luminal A–like and four from luminal B–like to triple-negative. No metastatic patients were initially luminal A–like. Changes in subtype were associated with tumor histologic grade: 10 (66.7%) grade 1 tumors changed subtype, versus six (20.7%) grade 2 and 11 (26.2%) grade 3 cases (p=0.005).

Changes in tumor immunohistochemical profiles in pre- and post-NACT samples from 86 invasive breast carcinomas (p < 0.001). HER2, human epidermal growth factor receptor 2; NACT, neoadjuvant chemotherapy.
The following tumor biomarkers were associated with a lower risk of death: ER-positive expression in pre- (HR, 0.35; 95% CI, 0.21 to 0.58; p < 0.001) and post-NACT (HR, 0.39; p < 0.001) tumor samples, PR positive expression in pre- (HR, 0.37; 95% CI, 0.20 to 0.63; p < 0.001) and post-NACT (HR, 0.57; 95% CI, 0.32 to 0.98; p=0.044) tumor samples. On the other hand, high Ki67 index in the initial biopsy (HR, 2.47; p=0.001) (Fig. 1A), Luminal B-like profile on post-NACT tumor sample (HR, 2.58; 95% CI, 1.09 to 6.13; p=0.031); and triple-negative profile in pre- (HR, 4.45; 95% CI, 2.12 to 9.32; p < 0.001) (Fig. 1B) and post-NACT tumor samples (HR, 4.52; 95% CI, 2.29 to 8.92; p < 0.001) (Fig. 1C) were associated with a higher risk of death. Any change in IHC tumor profile was associated with overall survival in log-rank test (p=0.050). In Cox-regression IHC changes showed a tendency to increase patients’ overall survival time, with a HR of 0.57 (95% CI, 0.33 to 1.01; p=0.054) (Fig. 1D).
In the multivariate analysis (Table 4), the pre-NACT tumor histologic grade III (p=0.021); and both pre- and post-NACT triple-negative IHC tumor profile (p=0.003 and p < 0.001) (Table 4) proved to be independent predictors of overall survival time.
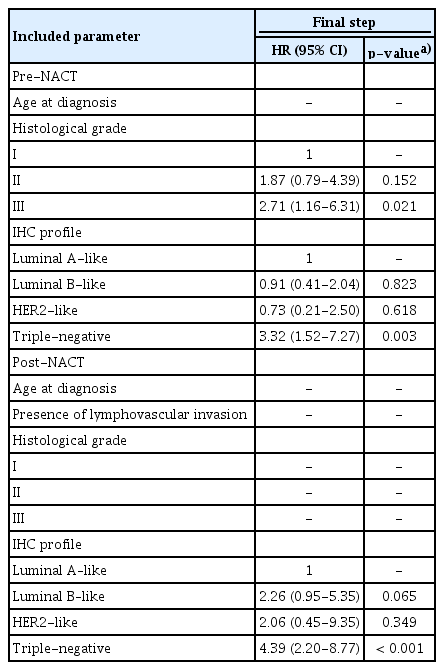
Clinicopathological characteristics of invasive breast carcinomas in pre- and post-NACT samples and multivariate survival analysis
Discussion
The changes in tumor pathological characteristics and biomarkers expression after neoadjuvant therapy are widely debated in the literature. They could directly affect decisions regarding adjuvant therapy [2,19].
In our study, 26 (30.2%) tumors changed the IHC subtype. The most frequent changes were from luminal B to luminal A-like subtype (46.2%) and from luminal B-like to triple-negative (27%). The post-NACT tumor IHC profile was still strongly associated with survival in comparison to the pre-NACT sample. Other studies also found post-NACT changes in 16% to 27.2% of cases, but some of them did not consider the Ki67 index in subtype IHC classification [4,20].
Interestingly, in our study, changes in IHC profile were marginally associated with longer overall survival time (HR, 0.57; 95% CI, 0.32 to 1.01; p=0.056). We believe this is due to the most common changes encountered, as lower Ki67 index, with a change from luminal B to luminal A–like breast cancer. The Ki67 index is a well-established proliferative marker predictive of response to chemotherapy [2,19]. In our study, nearly half of post-therapy residual tumors (42/86) had lower index of Ki67, representing more favorable clinical outcomes. Many other studies showed lower indexes of Ki67 after NACT [1,21]. Those changes may be due to therapy targeting proliferating cells [19]. Adjuvant hormonal and anti-HER2 therapies also may have influenced our survival results.
Positivity for estrogen and progesterone receptors predicts response to endocrine therapy. It also represents a lower risk of recurrence in short term [12]. Changes in estrogen and progesterone receptors status from positive to negative were significant. In the literature, similar results have been described, either turning from negative to positive or from positive to negative after NACT [2-4,7,20]. Reddy and Apple [1] described a worse prognosis when PR status changed to negative. On the other hand, Chatterjee et al. [22] described shorter survival time when hormone receptor negative tumors became positive after NACT.
HER2 changes can also occur after NACT. Only two cases lost HER2 overexpression, and curiously, one of them was equivocal (score 2+) at the initial biopsy [3,8]. Several studies found HER2 expression discordance, mostly losing expression after therapy, ranging from 9.8% to 24.7%, but in some of these studies patients were treated with anti-HER2 target therapy [3,4,7,20]. In our study, patients with HER2 positive tumors did not receive anti-HER2 therapy in the neoadjuvant setting and only one patient out of two cases that lost HER2 expression, received adjuvant anti-HER2 therapy. In our study, HER2 expression and changes after NACT were not associated with overall survival time. However, only 11 (12.8%) of our cases showed HER2 overexpression.
The dynamics of IHC changes is yet to be fully understood. Thus, it is debatable whether targeted treatment should be reviewed according to changes in IHC subtype after NACT. To our knowledge, no prospective randomized trials have been performed addressing this issue. Although there is still no consensus or guideline indicating biomarkers routine retesting in residual tumors [23], we are in accordance with previous authors who recommend that biomarkers should be retested, especially in hormone receptors or HER2-negative cases, since these could represent false-negative results in the initial biopsy [1-4,7,10,20,21].
Basically, two factors can explain changes in tumor characteristics before and after NACT: sampling differences in tumor biopsies versus resection specimens, and changes related to neoadjuvant treatment.
Tumor heterogeneity, small sampling of the initial biopsy, results close to the negative/positive limit, and false-negative initial results (pre-analytical and/or analytical factors) [1,24,25] have been described. We detected more in situ carcinomas and the presence of LVI in residual post-therapy samples than in pre-therapy samples. Core biopsies tends to represent the central area of the tumor, whereas these features predominate in the periphery of the tumor. These changes were significant in univariate analysis and are in accordance with previous studies [26]. Presence of LVI was not an independent predictor of survival time in multivariate analysis [7].
Changes in nuclear pleomorphism and mitotic index may be associated with chemotherapy effects on cells and tumor progression but have also been reported in surgical samples of patients who didn’t undergo neoadjuvant therapy, usually explained by sampling variability with a higher tumor grade in the resection specimen when compared to the initial core needle biopsy [27].
Histological type changes in residual tumors after NACT have also been described previously [24,25]. Our study included tumors with more than one histological type (mixed type) in the initial biopsy that showed only one special type in post NACT residual tumor, indicating that cell clones could be selected. However, other tumors with one pure special type changed to mixed types after surgical resection. These could represent true changes after NACT in histological tumor type or could have had an under representative tumor sample of a heterogeneous tumor reaching only part of the tumor [1,7]. Changes in histological type were not significant in this study.
In general, there is a good concordance with the percentage of tumor infiltrating inflammatory cells between the initial biopsy and the surgical resection tumors [28]. It is already known that a higher percentage of tumor infiltrating inflammatory cells predicts better response to chemotherapy. The increase in the percentage of these inflammatory cells after NACT is also associated with longer survival time, especially in triple-negative IBCs [21]. In this study, changes in the percentage of tumor infiltrating inflammatory cells were significant but did not influence the overall survival of our patients.
This study was conducted in a Brazilian public hospital. Our cases were diagnosed and treated at the same hospital, following the same therapy protocols. All histopathological slides were reviewed and analyzed by the same pathologist (C.B.N.). Although being a retrospective study, IHC tests were repeated, using the same protocol and antibodies. All assays were performed by the same person (B. J.S.), seeking standardization and to eliminate interpretation or technical biases. Unfortunately, our patients presented with advanced breast carcinomas. Most of them died during follow-up. Other studies have also shown that Brazilian patients are frequently diagnosed with advanced disease. They usually don’t have access to diagnosis and therapies in due time, which may explain our frequency of high stage disease and short overall survival time [29].
In conclusion, we found changes in tumor characteristics and biomarkers after exposure to NACT and showed that these changes can help predict a patient’s risk of death, tailoring adjuvant treatments. We suggest that tumors should be reclassified, regraded and IHC biomarkers should be retested on post-neoadjuvant residual tumors to improve therapeutic decisions.
Notes
Ethical Statement
This is a retrospective cohort study, approved by the Research Ethics Committee of the Federal University of Minas Gerais (COEPUFMG) under protocol # 2.109.565. Given the retrospective nature of the study, no informed consent was required from the research ethics committee.
Author Contributions
Conceived and designed the analysis: Santos BJ, Balabram D, Nunes CB.
Collected the data: Santos BJ, Gomes VMR, Castro CCC, Nunes CB.
Contributed data or analysis tools: Santos BJ, Balabram D, Diniz PH, Nunes CB.
Performed the analysis: Santos BJ, Balabram D, Buzelin MA, Nunes CB.
Wrote the paper: Santos BJ, Balabram D, Nunes CB.
Conflicts of Interest
Conflict of interest relevant to this article was not reported.
Acknowledgements
This work was supported in part by the Conselho Nacional de Desenvolvimento Científico e Tecnológico and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior.