Prevalence and Risk Factors of Germline Pathogenic Variants in Pancreatic Ductal Adenocarcinoma
Article information

Abstract
Purpose
The genetic attribution for pancreatic ductal adenocarcinoma (PDAC) has been reported as 5%–10%. However, the incidence of germline pathogenic variants (PVs) in Korean PDAC patients has not been thoroughly investigated. Therefore, we studied to identify the risk factors and prevalence of PV for future treatment strategies in PDAC.
Materials and Methods
Total of 300 (155 male) patients with a median age of 65 years (range, 33 to 90 years) were enrolled in National Cancer Center in Korea. Cancer predisposition genes, clinicopathologic characteristics, and family history of cancer were analyzed.
Results
PVs were detected in 20 patients (6.7%, median age 65) in ATM (n=7, 31.8%), BRCA1 (n=3, 13.6%), BRCA2 (n=3), and RAD51D (n=3). Each one patient showed TP53, PALB2, PMS2, RAD50, MSH3, and SPINK1 PV. Among them, two likely PVs were in ATM and RAD51D, respectively. Family history of various types of cancer including pancreatic cancer (n=4) were found in 12 patients. Three patients with ATM PVs and a patient with three germline PVs (BRCA2, MSH3, and RAD51D) had first-degree relatives with pancreatic cancer. Familial pancreatic cancer history and PVs detection had a significant association (4/20, 20% vs. 16/264, 5.7%; p=0.035).
Conclusion
Our study demonstrated that germline PVs in ATM, BRCA1, BRCA2, and RAD51D are most frequent in Korean PDAC patients and it is comparable to those of different ethnic groups. Although this study did not show guidelines for germline predisposition gene testing in patients with PDAC in Korea, it would be emphasized the need for germline testing for all PDAC patients.
Introduction
According to global cancer statistics, pancreatic cancer is the 14th most commonly diagnosed cancer worldwide and the seventh leading cause of cancer deaths because of its poor prognosis [1]. In Korea, pancreatic cancer is the eighth most common cancer and the fifth leading cause of death and the incidence of pancreatic cancer in all cancers has gradually increased from 2.3% in 2010 to 3.2% in 2019, with the lowest 5-year survival rate of 13.9% among major cancers [2].
Risk factors for pancreatic cancer include cigarette smoking, increased body mass index, diabetes, alcohol consumption, and chronic pancreatitis; pancreatic cancer is thought to have a familial component in approximately 10% of cases [3]. Moreover, BRCA1/2, PALB2, ATM, TP53, MLH1, STK11/LKB1, APC, CDKN2A, and SPINK1/PRSS1 are high-risk genes for pancreatic cancer [4].
Many solid organ cancers have clinical guidelines for evaluation and genetic counseling. However, many pancreatic cancer cases are diagnosed at an advanced stage because most patients have nonspecific symptoms, and there are no effective screening tools for pancreatic cancer. Notably, identifying carriers of cancer predisposition genes enables the identification of high-risk family members and their detection in the early stage of the disease [5]. Therefore, it is important to identify at-risk patients and screen them for early detection to improve the mortality rate of pancreatic cancer. The National Comprehensive Cancer Network (NCCN) guidelines recommend that clinicians consider germline testing in patients diagnosed with pancreatic cancer [6]. Pancreatic cancer is associated with numerous hereditary syndromes, including familial pancreatic cancer and germline; thus, testing is important [7]. If a cancer syndrome is identified, at-risk relatives should be offered genetic counseling and advised on risk-reducing strategies, including smoking cessation, weight loss, and screening for pancreatic and other cancers [4,8].
However, the prevalence of genetic predisposition and germline pathogenic variants (PVs) in Korean patients with pancreatic cancer has not been thoroughly investigated. This study aimed to identify the risk factors and prevalence of PV for future treatment strategies for pancreatic ductal adenocarcinoma (PDAC).
Materials and Methods
1. Patients
This study was a single-center study. Patients who visited the center for liver and hepatobiliary cancer and/or genetic counseling clinic at the Korea National Cancer Center were recruited from March 2017 to August 2022. All included patients were diagnosed with PDAC and underwent germline next generation sequencing (NGS) panel testing for cancer predisposition genes.
Data on demographics, personal and familial histories of cancer, and panel testing results were collected. Additionally, clinicopathological characteristics of cancer, such as stage, tumor location, treatment, and family history, were assessed by reviewing medical records. This study was approved by the International Review Board (IRB) of the National Cancer Center of Korea (IRB No. NCC2019-0034, NCC2021-0233, and NCC2021-0338). Clinical follow-up data were reviewed for treatment regimen and response, especially in the patients harboring PVs.
2. Multigene panel testing and interpretation
Genomic DNA was extracted from the peripheral blood of each patient. We employed a customized hereditary cancer panel (Celemics, Seoul, Korea) that included all coding sequences and intron-exon boundaries of the coding exons from 28 cancer predisposition genes (S1 Table). Nine patients who were recently involved in the study were analyzed for 73 cancer predisposition genes (including SPINK1). The libraries were prepared according to the manufacturer’s guidelines and sequenced on an Illumina MiSeqDX (Illumina Inc., San Diego, CA), generating 2×150 bp paired-end reads. Alignment of sequence reads, indexing of the reference genome (hg19), and variant calling were performed with a pipeline based on GATK Best Practice [9]. Alignment was performed with BWA-mem (ver. 0.7.10) [10], duplicated reads were marked with Picard (ver. 1.138, http://picard.sourceforge.net), and local alignment, base quality recalibration, and variant calling were performed using the Genome Analysis Tool kit (GATK, ver. 3.5) [11], samtools (ver. 0.1.19) [12], FreeBayes (v0.9.21-26-gbfd9832) [13], and Scalpel (ver. 0.5.3). Variant annotation was performed with a Variant Effect Predictor (VEP) [14] and dbNSFP) [15].
Genes associated with the location and type of pancreatic cancer are indicated as lollipops, and a schematic representation was generated using the mutation mapper tool in cBioPortal [16]. Genetic variants were classified using a five-tier system following the American College of Medical Genetics and Genomics guidelines as follows: pathogenic (P), likely pathogenic, variants of uncertain significance (VUS), likely benign, and benign [17].
3. Statistical analysis
To evaluate risk factors, the clinicopathological features of the patients were summarized according to the type of variables as frequency and percentage and median (min-maximum). For comparison according to germline PVs, the chi-square test or Fisher’s exact test was used for categorical variables, and the Wilcoxon rank sum test was performed for continuous variables. The Kaplan-Meier method was used to analyze progression-free survival (PFS) and overall survival (OS).
All statistical analyses were performed using SAS ver. 9.4 (SAS Institute Inc., Cary, NC), and a p-value < 0.05 was considered statistically significant.
Results
1. Clinicopathologic features of patients
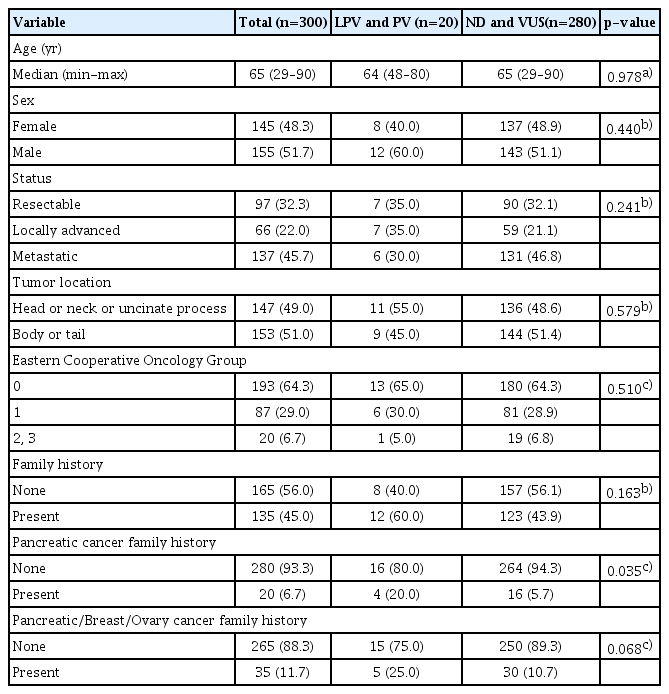
Overall, 300 patients diagnosed with PDAC were included in the current analysis. Detailed clinicopathological characteristics of the patients are summarized in Table 1. The median age at diagnosis was 65 years (range, 33 to 90 years), and 155 patients (51.6%) were men. Stages at initial diagnosis were resectable in 97 (32.3%), locally advanced in 66 (22.0%), and metastatic in 137 (45.7%) patients. Tumors were located in the head and neck of the pancreas in 147 patients (49.0%) and in the body and tail of the pancreas in 153 (51.0%). The completed pedigree for first-degree relatives was higher as n=70 compared to the second-degree relatives as n=25 by detailed pedigree evaluation. Acquired family history represented mean number (range) of relatives of first-degree and second-degree as 7.4 (3–13) and 6.3 (1–15), respectively. However, third-degree relative information was not available in all patients.
Comparison of clinicopathologic features between patient with and without germline PVs
2. PVs in patients
Among the 300 patients with PDAC, 20 had germline PVs (Fig. 1A). The mean age at diagnosis of the patients with germline PVs was 65 (range, 49 to 80), and 12 patients (60%) were men. There was no significant association between germline PVs and clinical features regarding age, sex, cancer stage, tumor location, and Eastern Cooperative Oncology Group performance status.

Germline variants in patients with hereditary pancreatic cancer detected using hereditary next generation sequencing (NGS) cancer panel testing. (A) Schematic representation of the patients and study workflow. A total of 300 pancreatic cancer patients were enrolled. Patients were enrolled in the study and testing using a hereditary NGS cancer panel testing. (B) The frequency of each germline pathogenic variants. (C) One patient had three germline pathogenic variants (BRCA2, MSH3, and RAD 51D). (D) Location and number of frequent pathogenic variants in four genes (ATM, BRCA1, BRCA2, and RAD51D) associated with pancreatic cancer. Locations of frequent pathogenic variants found in patients are shown with lollipop structures. The X-axis reflects the number of amino acid residues.
Detected germline PVs were ATM (n=7, 31.8%), BRCA1 (n=3, 13.6%), BRCA2 (n=3, 13.6%), RAD51D (n=3, 13.6%), TP53 (n=1, 4.5%), PALB2 (n=1, 4.5%), PMS2 (n=1, 4.5%), RAD50 (n=1, 4.5%), MSH3 (n=1, 4.5%), and SPINK1 (n=1, 4.5%) including two likely pathogenic variants (LPVs) in ATM and RAD51D, respectively (Fig. 1B). One patient had three germline PVs (BRCA2, MSH3, and RAD51D) (Fig. 1C). We checked the locations and frequencies of PVs in the four genes (ATM, BRCA1, BRCA2, and RAD51D). Fig. 1D illustrates the distribution of germline mutations in PDAC across the protein domains. Notably, no common founder mutations were found in these genes. Table 2 shows the detailed characteristics of patients with germline PVs. Twelve patients had various types of cancers in their families, and among them, three patients with ATM PVs and a patient with three germline PVs (BRCA2, MSH3, and RAD-51D) had first-degree relatives with pancreatic cancer.

Characteristics of patients with PVs
There were no significant differences between germline PVs and family history of various cancers; however, a family history of pancreatic cancer showed a significant difference (4/20, 20.0% vs. 16/264, 5.7%; p=0.035) (Table 1). Regarding the family history of either one of pancreas, breast, or ovarian cancer, the percentage of patients with germline PVs was higher; however, it did not reach a significant difference (5/20, 25.0% vs. 30/280, 10.7%; p=0.068). When we consider the frequency of genes of our study, it was comparable to the previous studies (S2 Table).
Among 20 PV and LPV patients, three patients were not affected by homologous recombination repair (HRR) gene mutation, and mutations in PMS2, SPINK1, and TP53 were identified as PV, respectively. Comparing the clinical factors of patients according to HRR gene mutation, it was confirmed that all variables related to family history were significantly different (S3 Table).
3. Progress and treatment of patients with PVs
Kaplan-Meier curves for PFS and OS according to disease status and presence of PVs were analyzed (Fig. 2A). The disease status showed significant differences in survival. PV harboring group represented PFS median (range) as 14.5 (0.3–49.7) compared to those not harboring PV as 9.1 (0.7–53.4). For OS, PV group vs. not detected or VUS group represented median survival as 21.6 (0.3–58.9) and 16.2 (0.7–75.3), respectively.
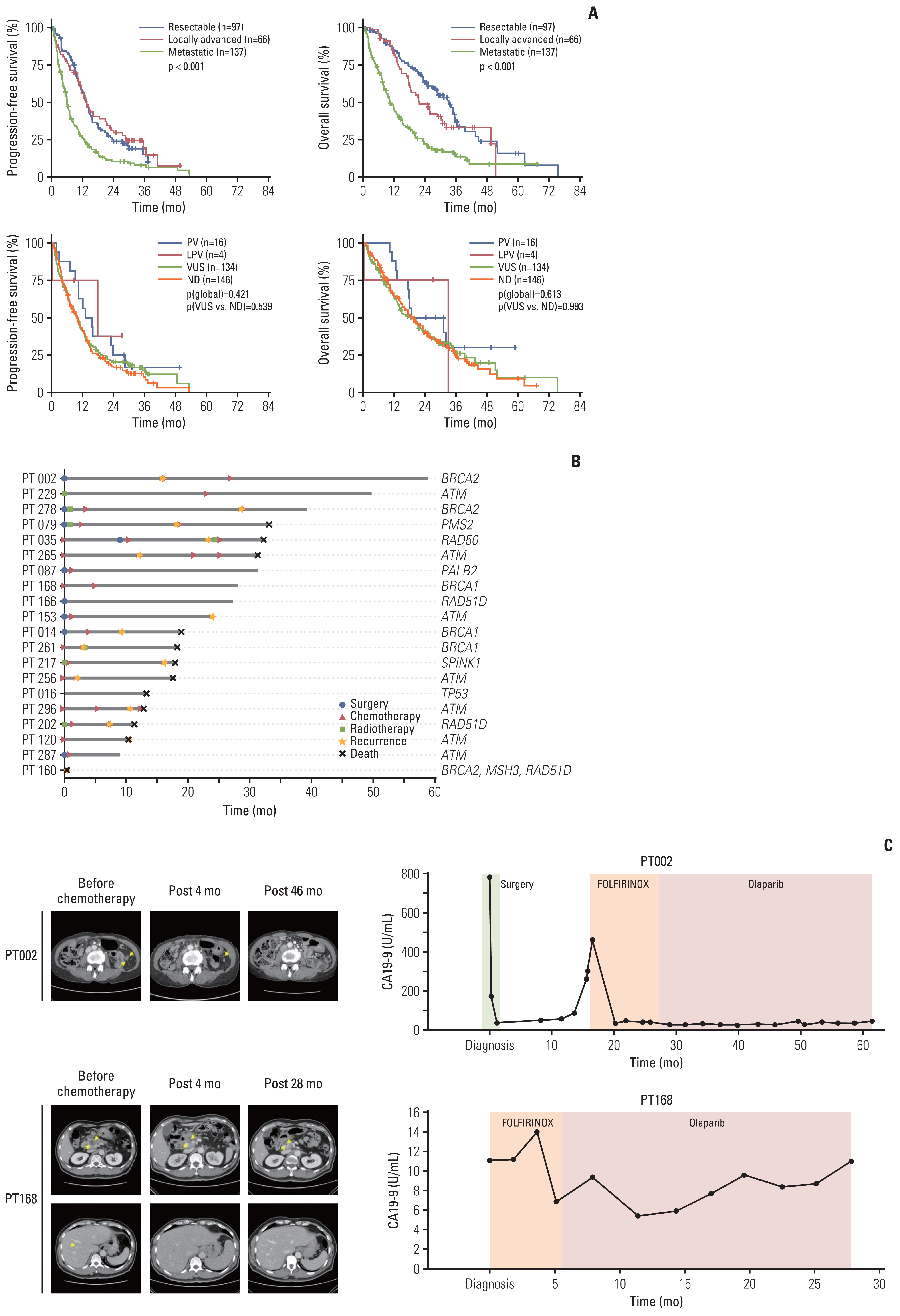
(A) Kaplan-Meier curves for progression-free survival and overall survival according to disease status and presence of pathogenic variants (PVs). The number of groups were represented as N. Median (range) survivals of progression-free survival and overall survival were as followings: resectable status (13.1 [0.7–37.3], 24.4 [0.7–75.3]) locally advanced status (13.0 [0.8–49.7], 21.4 [2.9–51.3]) and metastatic status (6.1 [0.3–53.4], 9.9 [0.3–67.2]). Germline mutations were grouped into four groups, such as PV, likely pathogenic variant (LPV), variants of uncertain significance (VUS), and not detected (ND), to determine if there was a difference in the progression-free survival and overall survival curves. It was confirmed that both progression-free survival and overall survival were not significant between the four groups. In addition, it was confirmed that there was no statistical difference in the survival curves of progression-free survival and overall survival between ND and VUS. (B) Progress of treatment and response of patients (n=20) with PVs. (C) PT002: A 51-year-old female underwent pancreatoduodenectomy had a recurrent tumor in the jejunum at the gastrojejunostomy site at 16 months. After 8 cycles of FOLFIRINOX (oxaliplatin, irinotecan, 5-fluorouracil, and leucovorin) treatment, the recurrent mass markedly decreased in size. After olaparib maintenance treatment, progression-free has been achieved up to 46 months with disappearance of the recurred tumor. PT168: A 65-year-old male suffered from weight loss with new-onset diabetes mellitus and was diagnosed as pancreatic cancer with multiple liver metastases. Liver biopsy confirmed moderately differentiated adenocarcinoma. After 8 cycles of FOLFORINOX treatment, pancreatic body cancer decreased in size from 27 mm to 13 mm and liver metastases were nearly invisible on follow-up computed tomography images indicating partial response. The patient received olaparib maintenance treatment, and the pancreatic body cancer further decreased in size to subcentimeter without liver metastases.
Two patients were treated by olaparib with relevance of genetic test. A 51-year-old female underwent pancreatoduodenectomy showed a recurred tumor at jejunum of gastrojejunostomy site with disease-free survival of 16 months. After 8 cycles of FOLFIRINOX (oxaliplatin, irinotecan, 5-fluorouracil, and leucovorin) treatment, recurred mass was markedly decreased. After olaparib maintenance treatment, progression-free have been achieved 46 months. The other suffered from weight loss with new-onset diabetes mellitus was diagnosed as pancreatic cancer with multiple liver metastases. After 8 cycles of FOLFIRINOX treatment, pancreatic body cancer decreased in size from 27 mm to 13 mm and liver metastases were nearly invisible on follow-up computed tomography images indicating partial response. Patients received olaparib maintenance treatment, and pancreatic body cancer further decreased in size to subcentimeter without liver metastases (Fig. 2B and C).
Discussion
Our study is the first to evaluate 28 gene sequences in a large number (n=300) of patients with PDAC in Korea. In this study, gene sequencing identified 20 variants in 300 patients (20/300, 6.7%) with PDAC. The germline PVs detected were ATM, BRCA1, BRCA2, RAD51D, TP53, PALB2, PMS2, RAD50, MSH3, and SPINK1. A family history of pancreatic cancer was significantly associated with germline PVs.
Much data on gene mutations in pancreatic cancer can be found for the Western and Asian population with a wide frequency range of 4%–18% [18–24]. Among PVs, BRCA1/2 and ATM mutations have been detected at a frequency of 18%–51% (this study, 27.2%), and 8%–30% (this study, 31.8%). Also, RAD51D mutations ranged in 0%–4.6% of PVs while our study 13.6%. It seemed our study has higher proportion of ATM and RAD51D gene mutations compared to the previous study. Though limited data were available for Asian populations, recent two studies from China and Japan reported a very similar percent of PVs as 6.2% (n=63/1,009) and 6.7% (n=67/1,005). In Korea, BRCA 1/2 mutations were detected in 10.0% (n=1/10) and 13.6% (n=9/66) of cases in small-scale study [25,26]. However, it seems overestimated considering our study result of 6.7% frequency. The common mutated genes ATM, BRCA1/2, and RAD51D were comparable to those reported in previous studies.
In Korea, genetic testing of BRCA1 and BRCA2 is recommended in context of reimbursement for the following patients with (1) diagnosed breast cancer and at least one family member or relative (within third-degree related) with breast cancer, ovarian cancer, male breast cancer, metastatic prostate cancer, or pancreatic cancer; (2) breast cancer diagnosed at age 40 or younger; (3) triple-negative breast cancer diagnosed at age 60 or younger; (4) bilateral breast cancer; (5) breast cancer with ovarian cancer or pancreatic cancer; (6) male breast cancer; and (7) ovarian cancer [27]. However, there are still no concrete recommendations of genetic testing for pancreatic cancer.
According to our study, those with a family history of pancreatic cancer showed a higher incidence of PVs (p=0.035). This finding highlights the importance of genetic testing in patients with a family history of pancreatic cancer, however, it is not solely applicable for the recommendation for genetic testing because only six of 20 patients (20%) with PVs presented pancreatic cancer family history. Moreover, acquisition of proper pedigree was difficult to complete up to third-degree relatives even when supported by a nurse. Our data revealed only 36% of counselee completed up to second-degree relatives in the overall pedigree overall.
One patient (PT002) with BRCA2 treated with olaparib as maintenance therapy showed 60 months survival at present and another patient (PT168) with BRCA1 also treated with olaparib, has been on follow-up 27 months until now. PDAC with BRCA1/2 gene mutation is not yet indicated for reimbursement of olaparib treatment in Korea. However, it would be considered in the near future for improvement of patient survival.
This study had some limitations. First, familial cancer history depended only on the recall of the patients; therefore, it may not be accurate and may be underestimated. Second, the number of germline PVs was not enough to confirm associations with clinical characteristics. Thus, further studies including larger numbers of PDAC patients are needed. Third, we did not analyze tissue NGS. Vidula et al. [28] identified that BRCA1/2 somatic and germline mutations frequencies different in cancer types of breast, ovarian, pancreatic, and prostate. Testing for somatic mutations may increase the ability to identify potential therapeutic options for patients over germline testing alone [29].
In conclusion, this study showed a 6.7% prevalence of germline PVs in Korean patients with PDAC. Although we still do not have guidelines for germline predisposition gene testing in patients with PDAC in Korea, such as the NCCN guidelines in the United States, our results showed that the incidence of PVs was comparable with that in other countries. Further analysis of a larger number of patients is needed to expand our knowledge of the incidence and involvement of genes involved in cancer predisposition in Korean patients with PDAC.
Electronic Supplementary Material
Supplementary materials are available at Cancer Research and Treatment website (https://www.e-crt.org).
Notes
Ethical Statement
This study was approved by the International Review Board (IRB) of the National Cancer Center of Korea (IRB No. NCC2019-0034, NCC2021-0233, and NCC2021-0338) and written informed consent was obtained from all participants.
Author Contributions
Conceived and designed the analysis: Ryu KH, Woo SM, Kong SY.
Contributed data or analysis tools: Ryu KH, Park S, Woo SM, Kong SY.
Wrote the paper: Ryu KH, Park S, Chun JW, Cho E, Choi J, Lee DE, Shim H, Kim YH, Han SS, Park SJ, Kong SY.
Conflicts of Interest
Conflict of interest relevant to this article was not reported.
Acknowledgments
This study was supported by the National Cancer Center, South Korea (Grant no. 2110181 and 1910190). We thank help of Min Kyeong Kim, Yena Kim, and Young Hwa Kang.