Intensified First Cycle of Rituximab Plus Eight Cycles of Cyclophosphamide, Doxorubicin, Vincristine, and Prednisolone with Rituximab Chemotherapy for Advanced-Stage or Bulky Diffuse Large B-Cell Lymphoma: A Multicenter Phase II Consortium for Improving Survival of Lymphoma (CISL) Study
Article information
 , Jin Seok Kim1, Won Seog Kim2, Hyeon Seok Eom3, Deok-Hwan Yang4, Sung Hwa Bae5, Hyo Jung Kim6, Jae Hoon Lee7, Suk-Joong Oh8,a), Sung-Soo Yoon9, Jae-Yong Kwak10, Chul Won Choi11, Min Kyoung Kim12, Sung Young Oh13, Hye Jin Kang14, Seung Hyun Nam15,b), Hyeok Shim16, Joon Seong Park17, Yeung-Chul Mun18, Cheolwon Suh19, The Korean Society of Hematology Lymphoma Working Party
, Jin Seok Kim1, Won Seog Kim2, Hyeon Seok Eom3, Deok-Hwan Yang4, Sung Hwa Bae5, Hyo Jung Kim6, Jae Hoon Lee7, Suk-Joong Oh8,a), Sung-Soo Yoon9, Jae-Yong Kwak10, Chul Won Choi11, Min Kyoung Kim12, Sung Young Oh13, Hye Jin Kang14, Seung Hyun Nam15,b), Hyeok Shim16, Joon Seong Park17, Yeung-Chul Mun18, Cheolwon Suh19, The Korean Society of Hematology Lymphoma Working PartyAbstract
Purpose
This phase II, open-label, multicenter study aimed to investigate the efficacy and safety of a rituximab intensification for the 1st cycle with every 21-day of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone (R-CHOP-21) among patients with previously untreated advanced-stage or bulky diffuse large B-cell lymphoma (DLBCL).
Materials and Methods
Ninety-two patients with stage III/IV or bulky DLBCL from 21 institutions were administered 8 cycles of R-CHOP-21 with an additional one dose of rituximab intensification on day 0 of the 1st cycle (RR-CHOP). The primary endpoint was a complete response (CR) rate after 3 cycles of chemotherapy.
Results
Among the 92 DLBCL patients assessed herein, the response rate after 3 cycles of chemotherapy was 88.0% (38.0% CR+50.0% partial response [PR]). After the completion of 8 cycles of chemotherapy, the overall response rate was observed for 68.4% (58.7% CR+9.8% PR). The 3-year progression-free survival rate was 64.0%, and the 3-year overall survival rate was 70.4%. Febrile neutropenia was one of the most frequent ≥ grade 3 adverse events (40.0%) and five treatment-related deaths occurred. Compared with the clinical outcomes of patients who received R-CHOP chemotherapy as a historical control, the interim CR rate was higher in male patients with RR-CHOP (20.5% vs. 48.8%, p=0.016).
Conclusion
Rituximab intensification on days 0 to the 1st cycle of the standard 8 cycles R-CHOP-21 for advanced DLBCL yielded favorable response rates after the 3 cycles of chemotherapy and acceptable toxicities, especially for male patients (ClinicalTrials.gov ID: NCT01054781).
Introduction
Although the treatment outcomes of diffuse large B-cell lymphoma (DLBCL) have been improved with rituximab [1–3], up to 40% of DLBCL patients with advanced-stage or bulky disease are still resistant to current standard R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone) treatment [1,4,5]. Furthermore, salvage treatment has still yielded unsatisfactory results because > 70% of relapsed or refractory DLBCL patients do not present sustained survival after current salvage therapy, including autologous hematopoietic stem cell transplantation (ASCT) [6]. Therefore, a more effective first-line treatment strategy is required to overcome the limitations of R-CHOP among high-risk DLBCL patients.
Although R-CHOP every 21 days (R-CHOP-21) is generally used in high-risk DLBCL patients, the optimal dose and schedule of rituximab applications still have been investigated. Previous pharmacokinetic studies have revealed that the concomitant application of CHOP and rituximab does not achieve a plateau trough level of rituximab during the early cycles of chemotherapy, especially for elderly male patients. It was related to the rapid rituximab clearance in elderly male patients [7]. To improve the outcomes of R-CHOP chemotherapy for high-risk DLBCL patients, it is important to achieve appropriate serum concentrations of rituximab quickly. Here, we hypothesized that appropriate, therapeutic serum rituximab levels can potentially be achieved earlier by increasing the frequency and dose of rituximab applications, and then we can get a better treatment outcome. In this trial, the modifying regimen of rituximab administration with an additional one application on 1 day before (day 0) the 1st cycle of the R-CHOP-21 was tested for patients with high-risk DLBCL. If additional rituximab supplementation can appropriately increase the serum levels of rituximab, it may potentially improve the treatment outcomes of high-risk DLBCL patients.
Thus, in this prospective phase II study, we attempted to investigate the efficacy and safety of an intensification of rituximab on day 0 of the 1st cycle to the standard 8 cycles of R-CHOP-21 (RR-CHOP) chemotherapy in previously untreated DLBCL patients with stage III/IV or bulky disease.
Materials and Methods
1. Study design
Twenty-one institutions participated in this non-randomized, multicenter, prospective, open-label, phase II study in Korea [8]. This clinical trial was approved by the institutional review boards and ethics committees of each participating institution. The trial is registered on the National Cancer Institute website (trial number NCT01054781).
2. Patient eligibility
Eligible patients were aged > 18 years with histologically confirmed Ann Arbor stage III/IV, CD20-positive, newly diagnosed DLBCL, and/or bulky (largest diameter ≥ 10.0 cm) disease regardless of the stage [4]. Patients with primary central nervous system lymphoma, transformed DLBCL from indolent lymphoma, and a history of human immunodeficiency virus and hepatitis C virus infection were ineligible. Patients with hepatitis B virus (HBV)–seropositivity were eligible. However, primary prophylaxis with appropriate antiviral agents (i.e., lamivudine or entecavir) was recommended for HBV carriers to prevent HBV reactivation throughout the treatment period.
3. Treatment regimen
The R-CHOP-21 regimen, comprising rituximab (375 mg/m2; intravenous), cyclophosphamide (750 mg/m2; intravenous), doxorubicin (50 mg/m2; intravenous), and vincristine (1.4 mg/m2; maximum 2.0 mg intravenous) on day 1 and prednisone (100 mg/day; oral) on days 1–5, was administered. Additional rituximab (375 mg/m2; intravenous) was administered on 1 day (day 0) before the 1st cycle to 8 cycles of R-CHOP-21 (RR-CHOP). Although the granulocyte colony-stimulating factor (G-CSF) administration was not routinely used for primary prophylaxis, the therapeutic purpose of G-CSF was administered at the discretion of individual physicians. Radiotherapy or ASCT was administered after the completion of 8 cycles of R-CHOP at the discretion of each participating institution. Indications for radiotherapy after the completion of chemotherapy included bulky disease (≥ 10 cm) at diagnosis, localized positron emission tomography (PET)–positive lesions, and potential curability via radiotherapy.
4. Baseline evaluation and response assessment
Baseline evaluation was carried out for ≤ 28 days before enrollment, and all patients were staged by the Ann Arbor staging system, which included history-taking; physical examination; complete blood count; serum chemistry, including lactate dehydrogenase; bone marrow aspiration and biopsy; computed tomography; and PET imaging. Immunohistochemically defined sub-classification of DLB-CL, including germinal center B-cell type (GCB) and non–germinal center B-cell type (non-GCB), was recommended at each institution by the Hans algorithm [9].
All patients underwent response evaluation after 3 cycles, 6 cycles of R-CHOP, and approximately 4 weeks after the completion of treatment, in accordance with the international workshop criteria [10]. Safety profiles were evaluated by the National Cancer Institute Common Terminology Criteria for Adverse Events ver. 3.0 until the 30th day after the final cycles of chemotherapy. The highest grade during the courses of treatment was considered for analysis. Physical examination and basic laboratory analyses were conducted every 6 months. Tumor assessment was carried out every 3 months during the first 2 years and every 6 months during years 3 to 5.
5. Statistical analysis
The primary endpoint was the rate of complete response (CR) after 3 cycles of R-CHOP chemotherapy, and the secondary endpoints were the overall response rate (ORR), progression-free survival (PFS), overall survival (OS), and safety. PFS was defined as the time from treatment initiation to the first recording of relapse or disease progression or death from any cause. OS was defined as the time from initial treatment to death from any cause or the date of the final follow-up evaluation. To compare the efficacy of RR-CHOP, the clinical outcomes of R-CHOP–treated DLBCL patients as historical controls were analyzed, and propensity score matching was performed using a 1:1 matching protocol without replacement. Among 403 newly diagnosed DLBCL patients at Severance Hospital during the period from 2010 to 2013, 14 patients who were transferred to another hospital or did not receive any first-line chemotherapy were excluded. Of the remaining 389 patients, 197 patients with high-risk DLBCL according to the same inclusion criteria of this study were selected for historical control. Actuarial survival analysis and comparisons were carried out using the Kaplan-Meier method and the log-rank test. A Cox regression model was used to determine the hazard ratios and 95% confidence intervals. Statistical analysis was performed using SPSS ver. 25.0 (IBM Corp., Armonk, NY), and a p-value of < 0.05 was considered statistically significant.
Results
1. Patients characteristics
Between January and December 2009, 92 patients with newly diagnosed advanced-stage or bulky DLBCL were enrolled in this study. Fifty-two patients (56.5%) were older than 60 years (median 63, range 20 to 79 years), 14 (15.2%) had a European Cooperative Oncology Group poor performance status ≥ 2, and 85 (92.4%) had stage III/IV disease. Patient characteristics are summarized in Table 1.
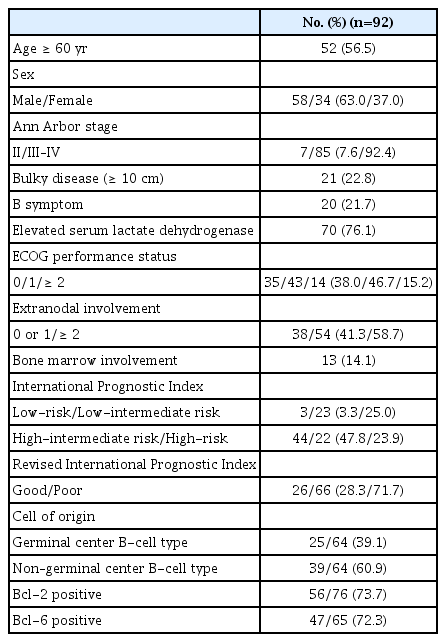
Patient characteristics
2. Treatment outcomes
The median number of RR-CHOP cycles was 8 (range, 1 to 8). Sixty-five patients (70.7%) completed 8 cycles of treatment following the protocol. CR rate and ORR after 3 cycles of RR-CHOP chemotherapy, were 38.0% (35/92) and 88.0% (81/92) in the full analysis set. Among the 92 patients initially enrolled herein, response data were not available for 10 patients after 3 cycles (3 died early, 3 were transferred to another institution, and 4 progressed disease). Based on the per-protocol analysis, the CR and ORR after 3 cycles of chemotherapy were 42.7% (35/82) and 98.8% (81/82), respectively. After the completion of 8 cycles of chemotherapy, 65 patients were assessed for the final response (Fig. 1).
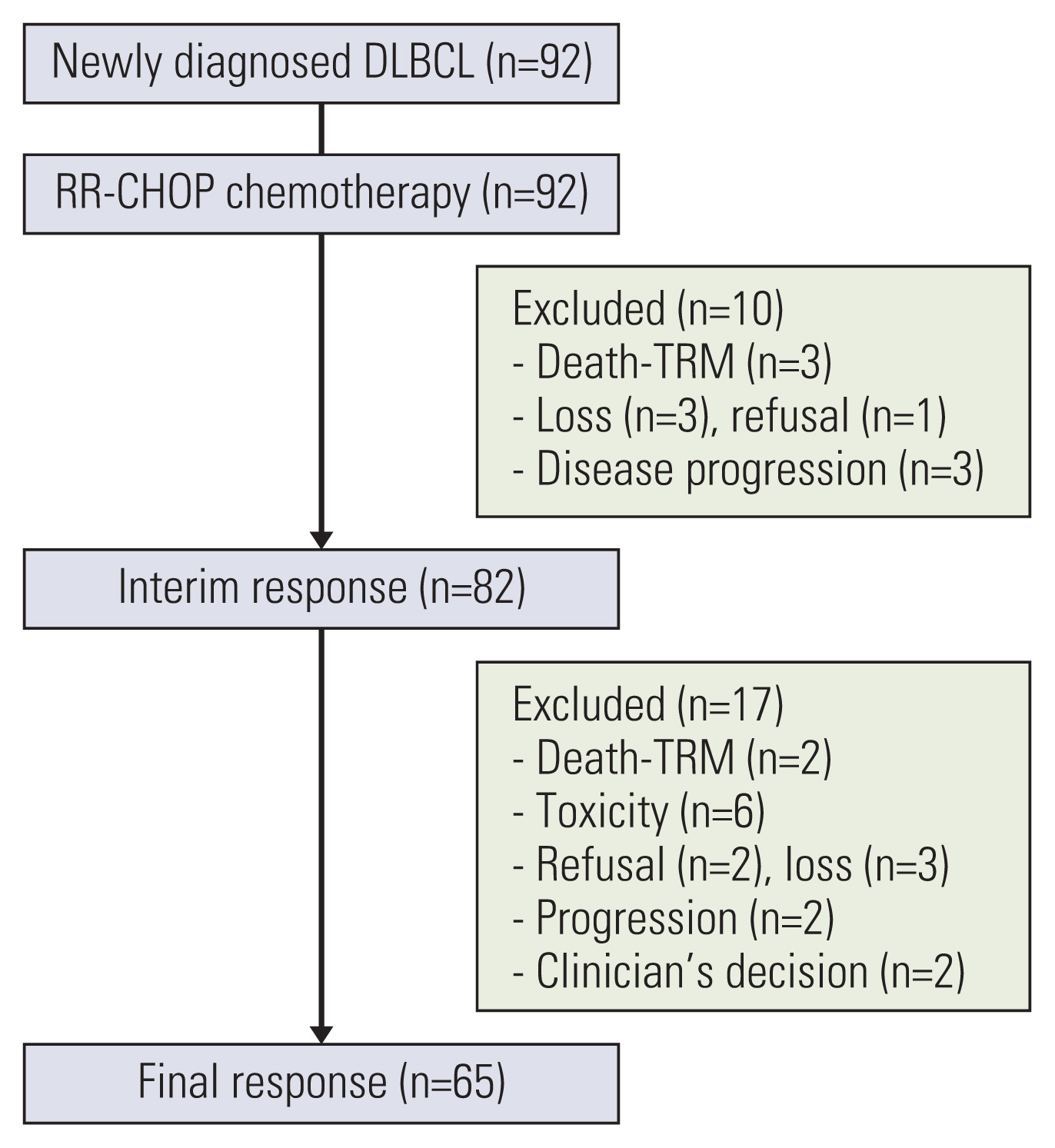
Diagram of the enrolled diffuse large B-cell lymphoma patients. DLBCL, diffuse large B-cell lymphoma; RR-CHOP, intensified the first cycle of rituximab plus eight cycles of cyclophosphamide, doxorubicin, vincristine, and prednisolone with rituximab; TRM, treatment-related mortality.
The reasons for 17 patients with discontinuation of chemotherapy after interim response analysis were as follows: two patients withdrew their consent, two died early, two presented disease progression, six presented treatment-related toxicities, three were lost to follow-up, and two were excluded according to the clinician’s discretion (Fig. 1). Fifty-four patients (58.7%) achieved a CR, nine (9.8%) achieved a partial response (PR), one achieved a stable disease and one (1.1%) presented with disease progression after the completion of 8 cycles of treatment (n=65). Based on the per-protocol analysis, the CR and ORR after 8 cycles of chemotherapy were 58.7% (54/65) and 96.9% (63/65), respectively. Among the 65 patients who completed the 8 cycles of RR-CHOP treatment, consolidative radiotherapy after the RR-CHOP chemotherapy was administered in four patients (6.1%) for the following indications: a bulky disease at initiation of treatment (n=1), consolidation at lymph nodes (n=2), or bone lesions (n=1). Ten patients received ASCT as consolidation: six patients received ASCT in a PR state and four patients received ASCT in a CR state.
3. Survival
The median follow-up duration for all patients was 36 months, and median PFS and OS were not reached. The 2-year and 3-year OS were 77.8% and 69.7%, respectively (Fig. 2A). The 2-year and 3-year PFS were 67.2% and 63.3%, respectively (Fig. 2B). No significant differences were obser-ved according to the international prognostic index (IPI), and the 3-year OS and PFS of low-risk patients were 100% and 100%, of low-intermediate risk patients were 81.1% and 76.5%, of high-intermediate risk patients was 64.8% and 60.4%, and of high-risk patients was 63.6% and 50.3% (p=0.412 and p=0.084, respectively). The OS of patients with a good revised IPI was not different from that of patients with a poor revised IPI (p=0.110), and PFS was better in patients with a good revised IPI (p=0.038). None of the factors affected the differences in survival via univariate analysis (Table 2). The OS and PFS were not significantly different according to sex (S1 Fig.).
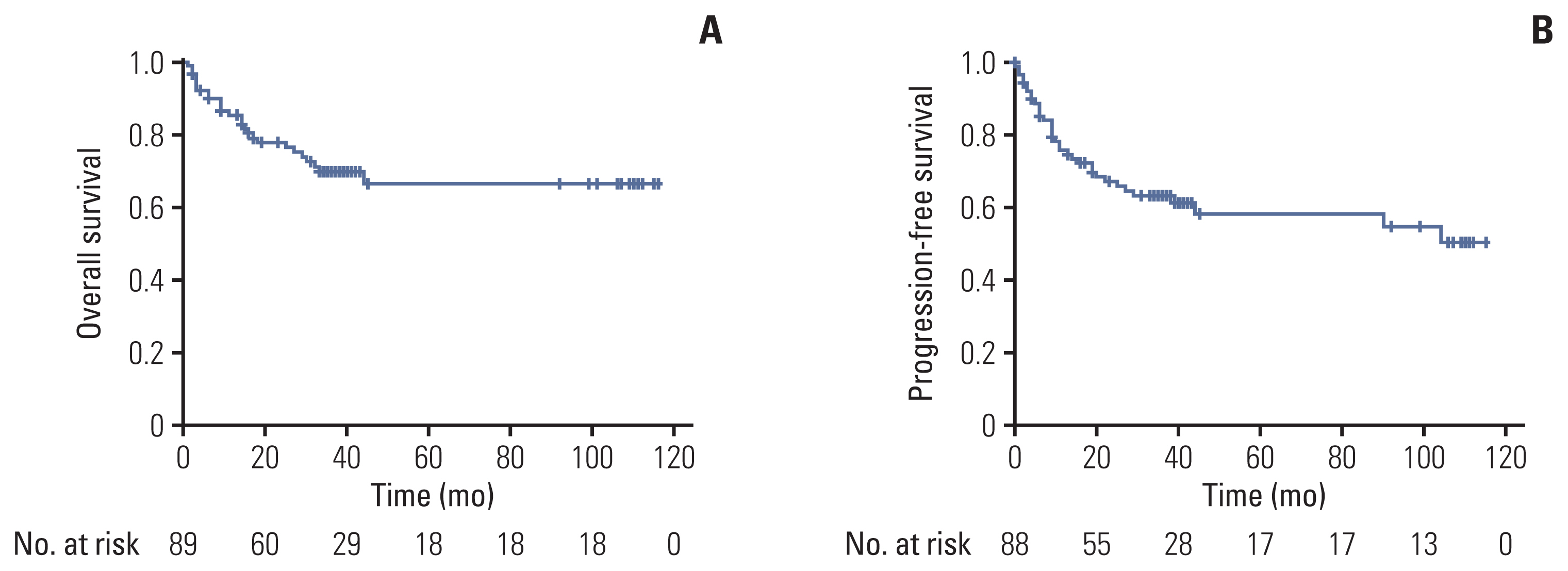
Kaplan-Meier analyses of overall survival (A) and progression-free survival (B) of patients receiving RR-CHOP chemotherapy. RR-CHOP, intensified the first cycle of rituximab plus eight cycles of cyclophosphamide, doxorubicin, vincristine, and prednisolone with rituximab.

Univariate analysis for overall survival and progression-free survival
4. Safety
Hematologic toxicities over grade 3 were the most common, with 67.0% neutropenia, 19.3% anemia, and 13.6% thrombocytopenia. Neutropenic fever was reported in 40% of patients, with three patients being grade 5. During RR-CHOP chemotherapy, a total of five treatment-related deaths occurred. Grade ≥ 3 non-hematologic toxicities included the following: generalized weakness (7.9%), anorexia (4.5%), abdominal pain (2.2%), diarrhea (2.2%), and lung toxicity (2.2%). Toxicity profiles (grade ≥ 3) during chemotherapy are summarized in Table 3.

Grade 3 to 5 AEs
5. Comparison with R-CHOP as a historical control
We compared the treatment outcomes of RR-CHOP chemotherapy with those of patients who received R-CHOP chemotherapy. Among 197 high-risk DLBCL patients treated with R-CHOP, 72 age, and IPI-matched patients were selected from each group (S2 Table). The 90.2% (43.1% [31/72] CR+47.2% [34/72] PR) of ORR after 3 cycles of RR-CHOP chemotherapy was superior to 83.3% of ORR (25.0% [18/72] CR and 58.3% [42/72] PR) in patients with R-CHOP (p=0.042). After the completion of planned chemotherapy, the final response was able to be assessed in 65 patients with the R-CHOP group. Thirty-four patients (47.2%) achieved CR, 18 (25.0%) achieved PR, and four (5.6%) patients progressed disease in the R-CHOP group. A higher CR rate (59.7%, 43/72) was observed in the patients who received RR-CHOP compared to the patients who received R-CHOP (47.2%, 34/72, p=0.041). The interim CR rate for male patients in the RR-CHOP group was significantly higher than that in the R-CHOP group (48.8% [21/43] vs. 20.5% [9/44], p=0.016). However, the final CR rate was not different between the two groups (55.8% [24/43] vs. 50.0% [22/44], p=0.209) (S3 Table). The OS and PFS were not significantly different between the two groups (S4 Fig.). The OS and PFS according to the two treatment groups also were not significantly different in both male and female patients (S5 Fig.). The OS and PFS according to the two treatment groups also were not significantly different in both younger (age 18–65 years) and older (age > 65 years) patients (S6 Fig.).
Discussion
This multicenter, prospective, phase II study including patients with newly diagnosed advanced-stage or bulky DLBCL treated with RR-CHOP revealed a favorable CR rate after 3 cycles of chemotherapy in comparison with historical risk-matched patients who were treated with R-CHOP. In particular, the RR-CHOP group displayed higher interim CR rates for male patients compared to the patients who received R-CHOP. These results showed that rituximab intensification on the standard R-CHOP chemotherapy has a meaningful clinical activity for some sub-groups of DLBCL patients.
There is a consensus that improvements in the outcomes of R-CHOP for advanced-stage DLBCL patients would warrant another treatment strategy. Dose-dense regimens, or dose-intense regimens, including additional use of etoposide, did not improve clinical outcomes in DLBCL [11,12]. Additional use of new investigational drugs such as bortezomib, bevacizumab, lenalidomide, and ibrutinib to the R-CHOP chemotherapy also did not improve the survival outcomes of DLBCL patients [13–16]. Early intensification and prolonged rituximab exposure in the SMARTE-R-CHOP-14 trial (6 cycles of CHOP-14 combined with 8 doses of rituximab on days −4, −1, 10, 29, 57, 99, 155, and 239), improved outcomes among elderly poor-prognosis patients compared to the historical control group who received R-CHOP from the RICOVER-60 trial [3,17]. DENSE-R-CHOP-14 trial (12 doses of rituximab was given on days 0, 1, 4, 8, 15, 22, 29, 43, 57, 71, 85, and 99 together with 6 cycles of CHOP-14 cycles) did not show improved outcomes compared to the historical control group from the RICOVER-60 trial and a higher incidence of infection was reported [18]. HOVON-84 study compared the RR-CHOP-14 regimen (R-CHOP-14 with the intensification of rituximab on day 8 of the first 4 cycles) and standard R-CHOP-14 regimen and early rituximab intensification of RR-CHOP-14 regimen did not show the survival benefit [19]. These studies suggest that earlier intensive use and longer exposure of rituximab may achieve the earlier higher and appropriate serum levels of rituximab, but the efficacy and clinical outcomes of additional use of rituximab to the R-CHOP regimen should be re-evaluated in further trials.
Because the clinical outcomes between R-CHOP-14 and R-CHOP-21 were not different, R-CHOP-21 is usually recommended as the first-line treatment in patients with DLBCL [20–22]. Therefore, previously reported intensified rituximab-containing regimens should be re-evaluated in the setting of the R-CHOP-21 backbone. Although the JCOG0601 trial compared the efficacy and safety of CHOP-21 plus dose-dense weekly rituximab (RW-CHOP-21) regimen with standard R-CHOP-21 regimen for DLBCL, the RW-CHOP-21 regimen did not show the improved PFS. This RW-CHOP-21 regimen was just a modification of the rituximab administration schedule (early intensification of rituximab during chemotherapy) and the total dose of rituximab during chemotherapy was the same between the two groups [23].
We added only one dose of rituximab on day 0 of the 1st cycle to the conventional 8 cycles R-CHOP-21 regimen in this trial for promptly achieving the appropriate serum level of rituximab and avoiding the further development of serious infections related to additional intensive use of rituximab. Considering the patients included in this study were high-risk, the CR or ORR after 3 cycles of RR-CHOP was comparable to the previous study [22].
Upon comparing patients receiving R-CHOP therapy in the historical control group, additional rituximab administration on day 0 of the 1st cycle of R-CHOP resulted in a higher interim CR among male patients in this study. Some studies have reported that male patients displayed inferior outcomes of conventional R-CHOP therapy [7,24,25]. Epidemiological studies have suggested that women have a survival advantage over men in various cancers [26,27]. Studies from the United States also have reported that male patients with lymphoma are at a higher mortality risk than female patients [26]. In DLBCL, elderly male patients benefit less from R-CHOP than female patients [7,24,28]. Elderly male DLBCL patients showed low serum levels of rituximab and inferior clinical outcomes of R-CHOP chemotherapy because of the rapid rituximab clearance. Intensified dose of rituximab (500 mg/m2) with CHOP-14 for elderly male patients showed similar PFS and OS to female patients, without increasing the toxicities [29]. The infection rate of RR-CHOP was slightly higher than that previously reported, but most cases were manageable in this study. Because prophylactic pegylated G-CSF is commonly recommended and used for the R-CHOP regimen in most countries, we can reduce the incidence of infection and cytopenia related to the RR-CHOP regimen after applying the prophylactic pegylated G-CSF. Therefore, rituximab intensification on day 0 of the 1st cycle to the standard 8 cycles of R-CHOP therapy is a potentially valuable alternative for advanced-stage high-risk DLBCL patients, especially for male DLBCL patients. This strategy can be easily applied in daily practice before getting the available newly approved first-line therapy for advanced-stage high-risk DLBCL patients such as polatuzumab vedotin-containing regimens [30].
The limitations of our study include the lack of a central pathological and radiological review. Furthermore, the study also involved inherent limitations associated with single-arm phase II studies having the response rate as the primary endpoint, such as small sample sizes and selection bias, which should be considered when interpreting the results. We stratified high-risk patients only based on clinical factors, not considering gene expression profiles, including those of cells expressing MYC or BCL2. However, clinical factors are more easily accessible in daily practice. Moreover, we did not carry out a pharmacokinetic analysis; this will be conducted in the future based on the present results.
This phase II study with an additional one dose of rituximab application on day 0 of the 1st cycle to 8 cycles of R-CHOP-21 for advanced-stage DLBCL revealed a favorable response, PFS, and OS, with acceptable toxicity. Moreover, rituximab intensification during early R-CHOP-21 therapy for male high-risk DLBCL patients might be an important treatment alternative.
Electronic Supplementary Material
Supplementary materials are available at Cancer Research and Treatment website (https://www.e-crt.org).
Notes
Ethical Statement
This study was conducted in accordance with the ethical standards of the institutional and national research committee and the Declaration of Helsinki. The study protocols were approved by the institutional review board of each center. This trial was registered on http://www.clinicaltrials.gov with the identifier NCT01054781. All participants provided written informed consent before enrollment.
Author Contributions
Conceived and designed the analysis: Kim YR, Kim JS, Suh C.
Collected the data: Kim YR, Kim JS, Kim WS, Eom HS, Yang DH, Bae SH, Kim HJ, Lee JH, Oh SJ, Yoon SS, Kwak JY, Choi CW, Kim MK, Oh SY, Kang HJ, Nam SH, Shim H, Park JS, Mun YC, Suh C.
Contributed data or analysis tools: Kim YR, Kim JS, Kim WS, Eom HS, Yang DH, Bae SH, Kim HJ, Lee JH, Oh SJ, Yoon SS, Kwak JY, Choi CW, Kim MK, Oh SY, Kang HJ, Nam SH, Shim H, Park JS, Suh C.
Performed the analysis: Kim YR, Kim JS, Suh C.
Wrote the paper: Kim YR, Kim JS.
Critical revision of the manuscript for important intellectual content: Kim JS, Suh C.
Conflicts of Interest
Conflict of interest relevant to this article was not reported.
Acknowledgments
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. NRF-2022R1A2C1013495).