A Randomized Phase II Study of Irinotecan Plus Cisplatin with or without Simvastatin in Ever-Smokers with Extended Disease Small Cell Lung Cancer
Article information

Abstract
Purpose
This study evaluated whether an addition of simvastatin to chemotherapy improves survival in ever-smokers with extensive disease (ED)–small cell lung cancer (SCLC).
Materials and Methods
This is an open-label randomized phase II study conducted in National Cancer Center (Goyang, Korea). Chemonaive patients with ED-SCLC, smoking history (≥ 100 cigarettes lifetime), and Eastern Cooperative Oncology Group performance status of ≤ 2 were eligible. Patients were randomized to receive irinotecan plus cisplatin alone or with simvastatin (40 mg once daily orally) for a maximum of six cycles. Primary endpoint was the the 1-year survival rate.
Results
Between September 16, 2011, and September 9, 2021, 125 patients were randomly assigned to the simvastatin (n=62) or control (n=63) groups. The median smoking pack year was 40 years. There was no significant difference in the 1-year survival rate between the simvastatin and control groups (53.2% vs. 58.7%, p=0.535). The median progression-free survival and overall survival between the simvastatin arm vs. the control groups were 6.3 months vs. 6.4 months (p=0.686), and 14.4 months vs. 15.2 months, respectively (p=0.749). The incidence of grade 3–4 adverse events was 62.9% in the simvastatin group and 61.9% in the control group. In the exploratory analysis of lipid profiles, patients with hypertriglyceridemia had significantly higher 1-year survival rates than those with normal triglyceride levels (80.0% vs. 52.7%, p=0.046).
Conclusion
Addition of simvastatin to chemotherapy provided no survival benefit in ever-smokers with ED-SCLC. Hypertriglyceridemia may be associated with better prognosis in these patient population.
Introduction
Small cell lung cancer (SCLC) constitutes 15% of newly-diagnosed lung cancer and 70% of this tumor presents as extensive disease at the time of diagnosis [1]. Extensive-disease (ED) SCLC is highly chemosensitive but rapidly progressing and resistant to chemotherapy and thus has very poor prognosis with a median survival time of 10 months [2]. For several decades, a combination of etoposide and platinum has been considered the standard treatment for ED-SCLC [2]. There is an urgent need for innovative treatments for providing survival benefits to these patients.
Statins are drugs that inhibit the conversion of 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) to mevalonate by inhibiting HMG-CoA reductase. These inhibitors are prescribed to reduce blood low-density lipoprotein–cholesterol (LDL-C) levels. Although these drugs are mostly used to decrease the risk of cardiovascular diseases, growing evidence has suggested that these drugs may play a possible role in cancer prevention and treatment [3–5]. In a preclinical study, statins demonstrated potent anti-tumor activity in suppressing the growth of cancer cells, inducing apoptotic cell death, and inhibiting angiogenesis and metastasis [6]. We also previously found that simvastatin enhances irinotecan-induced apoptosis through inhibition of proteasome in non-SCLC cells [7]. Additionally, a few epidemiological studies demonstrated that the risk of lung cancer or colorectal cancer is significantly lower in stain-users compared to non-statin users [8,9]. In a preclinical study with SCLC cells, statins inhibited tumor growth, stimulated cell apoptosis, and increased drug sensitivity to etoposide [10]. Based on the encouraging preclinical and early clinical anti-tumor effect of statin, we previously conducted a single-arm phase II study to evaluate the efficacy and toxicity of combination treatment with simvastatin plus irinotecan and cisplatin (IP) in 61 chemonaive patients with ED-SCLC [11]. Although the addition of simvastatin to chemotherapy did not improve the survival time in all the patients with ED-SCLC, synergistic efficacy was proven in heavy smokers with ED-SCLC. Ever-smokers with more than 65 pack-years showed significantly longer overall survival (OS) than ever-smokers with less than 65 pack-years or never-smokers (20.6 months vs. 10.6 months vs. 9.0 months, respectively; p=0.032) [11]. Thus, we designed this randomized phase II study to validate the exploratory results of a previous phase II study. This study aimed to evaluate whether a combination of simvastatin and IP improves the clinical outcomes of ever-smokers with ED-SCLC.
Materials and Methods
1. Patients
This single-center, prospective, open-label, randomized, phase II study was conducted at the National Cancer Center Korea (Goyang, Republic of Korea) (Clinical trial information: NCT01441349). Eligibility criteria were ≥ 18 years of age, cytologically or histologically confirmed SCLC, chemonaive extensive disease, smoking history with more than 100 cigarettes in their lifetime, performance status of ≤ 2 on the Eastern Cooperative Oncology Group (ECOG) scale, adequate organ function and normal hematologic function, and measurable tumor lesions according to the Response Evaluation Criteria in Solid Tumors (RECIST), ver. 1.1 [12]. Patients who had been on statin treatment before enrollment were excluded.
2. Study design and treatment
Eligible patients were randomized 1:1 into one of the two arms: IP alone or IP plus simvastatin. The patients were stratified by smoking pack-years (< 50 vs. ≥ 50 pack-years) and EGOG performance status (0 or 1 vs. 2). The IP group received 65 mg/m2 irinotecan and 30 mg/m2 cisplatin intravenously on days 1 and 8 every 3 weeks. The IP plus simvastatin group received 40 mg simvastatin orally daily and 65 mg/m2 irinotecan and 30 mg/m2 cisplatin intravenously on days 1 and 8 every 3 weeks. Simvastatin was administrated up to six cycles because we expected the synergistic effect of simvastatin and IP chemotherapy. All the treatments were continued until six cycles or the development of intolerable severe toxicity.
3. Tumor assessment
Tumors were assessed using computed tomography, magnetic resonance imaging, or positron emission tomography every 6 weeks until disease progression. The objective response rate (ORR) was defined as the number of patients who had a complete or partial response according to RECIST ver. 1.1 [12]. Adverse events were evaluated according to the Common Terminology Criteria for Adverse Events ver. 4.0.
4. Serum lipid and lipoprotein analysis
For exploratory analysis, serum samples were collected on day 1 of every cycle from all the patients. We measured the triglyceride levels using a free glycerol assay, high-density lipoprotein–cholesterol (HDL-C) using an enzymatic method, and LDL-C using a homogeneous enzyme immunoassay.
5. Statistical analysis
The primary endpoint was the 1-year survival rate after treatment. The expected 1-year survival rate after the IP treatment was 40%. This study was designed to detect a 20% increase in the 1-year survival rate following treatment with IP plus simvastatin, with a one-sided type I error rate of 10% and 80% power. With a 10% drop-out rate expected, the study sample size was set at 126 patients.
All the efficacy analyses were conducted in the intent-to-treat population. Adverse effects were analyzed only in the patients who received treatment. Pearson’s χ2 and Fisher’s exact tests were used to determine the relationships between the categorical variables where appropriate. The relationships between the categorical and continuous variables were tested using the t test. The significance of the changes in the continuous variables between the two groups was calculated using a two-sample t test. Progression-free survival (PFS) was calculated from the beginning of the study treatment to the first documentation of disease progression, death, or last follow-up visit. OS was calculated from the beginning of the study treatment to death or the final follow-up visit. The survival rate was estimated using the Kaplan-Meier method, and differences in the survival between the groups were assessed using the log-rank test. Cox proportional hazards models were used to calculate the survival hazard ratios (HRs). Two-sided p-values less than 0.05 were considered significant.
Results
1. Patient characteristics
Between September 16, 2011, and September 9, 2021, 125 patients were randomly assigned to receive either IP plus simvastatin (n=62) or IP (n=63) (Fig. 1). The median age of the patients was 64 years (range, 46 to 79 years), and male sex (n=116, 92.8%) was predominant (Table 1). The ECOG performance status of 2 was 41 (32.8%) and median body mass index (BMI) was 23.1 kg/m2 (range, 17.5 to 36.2 kg/m2). All the patients had a smoking history with a median of 40 (range, 2 to 108) pack-years. Patient characteristics were well-balanced between the treatment groups except for liver metastasis.

Consolidated Standards of Reporting Trials (CONSORT) study diagram.

Patient characteristics
2. Safety
A total of 125 patients were included in the safety evaluation. Patients received a median of 6.0 (range, 1.0 to 6.0) treatment cycles in both the IP plus simvastatin and control groups (p=0.832). The most common adverse effects were neutropenia (76.0%), diarrhea (58.4%), and anemia (56.0%) (Table 2). Grade 3 or worse adverse effects, which were reported in more than 5% of the patients, included neutropenia (49.6%), anemia (20.8%), and diarrhea (8.8%). No treatment-related deaths occurred in either treatment groups. There was no significant difference in any grade 3 or worse adverse event between the two treatment groups (62.9% in the IP plus simvastatin group vs. 61.9% in the IP group, p > 0.99). The addition of simvastatin to IP did not increase the incidence of grade 3 or higher neutropenia (53.2% vs. 46.0%), diarrhea (9.7% vs. 7.9%), or alanine transaminase increase (1.6% vs. 0.0%). However, the frequency of grade 3 or higher thrombocytopenia was significantly lower in the IP plus simvastatin group than in the IP group (0.0% vs. 11.1%, p=0.013).
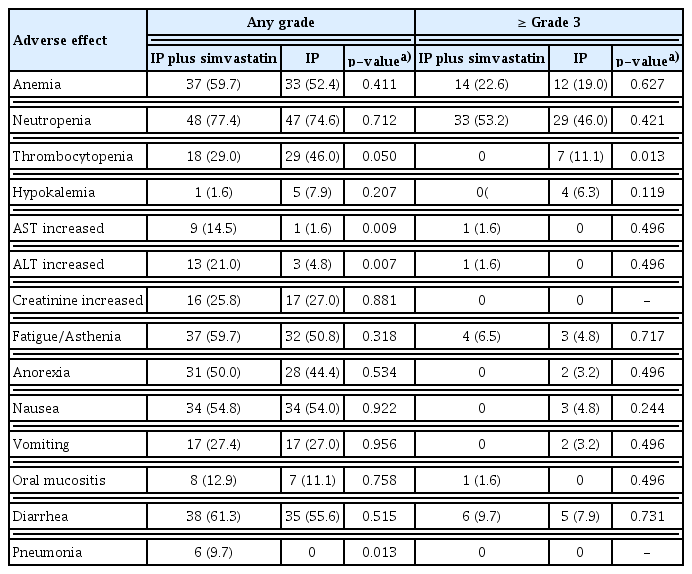
Summary of adverse effects
3. Efficacy
Considering the data cut-off on April 28, 2022, the median follow-up duration was 75.0 months and 119 patients (92.0) had experienced disease progression or death (Fig. 1). Three patients (4.8%) in the IP plus simvastatin group and three patients (4.8%) in the IP group were alive.
Tumor evaluation was available for 120 patients (96%). The ORR was not different between the two treatment groups (IP plus simvastatin, 54/61 [88.5%] vs. IP, 50/59 [84.7%]; p=0.543) (S1 Table).
The 1-year survival rates of the simvastatin and control groups were 53.2% and 58.7%, respectively (p=0.535). The IP plus simvastatin treatment did not prolong the PFS compared to the IP treatment alone (median PFS, 6.3 months [95% confidence interval (CI), 5.5 to 7.1] vs. 6.4 months [95% CI, 5.7 to 7.1]; HR, 1.07 [95% CI, 0.75 to 1.56]; p=0.686) (Fig. 2A). There was no significant difference in the OS between the IP plus simvastatin group and the IP group (median OS, 14.4 months [95% CI, 9.7 to 19.1] vs. 15.2 months [95% CI, 12.7 to 17.7]; HR, 1.06 [95% CI, 0.74 to 1.52]; p=0.749) (Fig. 2B).
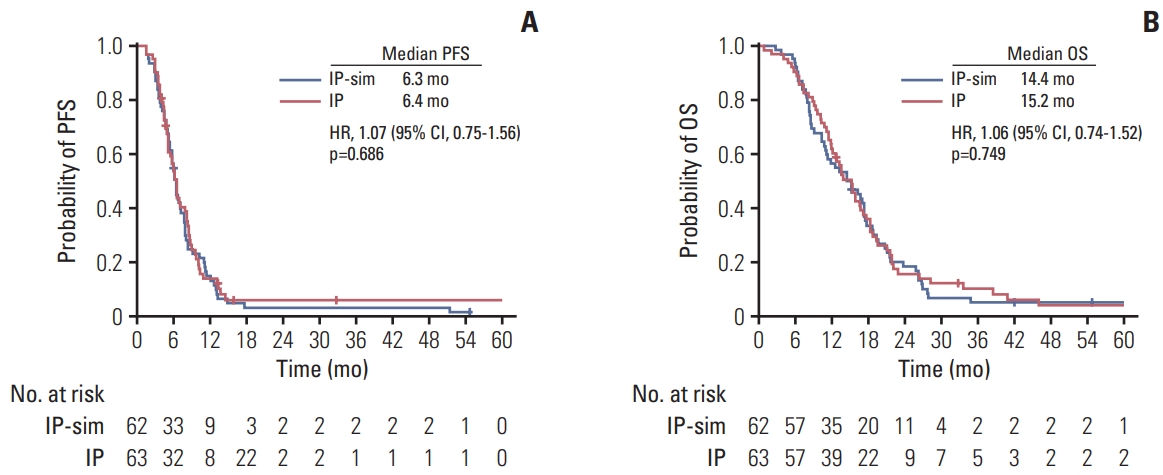
Kaplan-Meier curves: progression-free survival (PFS) (A) and overall survival (OS) (B). CI, confidence interval; HR, hazard ratio; IP, irinotecan plus cisplatin; IP-sim, irinotecan plus cisplatin and simvastatin.
After discontinuing the study, subsequent treatment was determined at the physician’s discretion (S2 Table). Subsequent systemic chemotherapy was administered to 47 of 62 patients (75.8%) in the IP plus simvastatin group and 46 of 59 patients (73.0%) in the IP group. Etoposide plus platinum regimen was mostly used in both the treatment groups (50.0% in the IP plus simvastatin group vs. 39.7% in the IP group, p > 0.99). Three (4.8%) patients in the simvastatin group and three patients (4.8%) in the IP group received immunotherapy with anti–programmed death-ligand 1 inhibitor.
The subgroup analysis for the PFS and OS was performed according to important clinical factors, including smoking pack year, BMI, serum lactate dehydrogenase (LDH), and lipoproteins (S3 Table). No subgroups showed a survival benefit from the addition of simvastatin to IP treatment. Even in the subgroup with more than 50 pack-years, no survival improvement was observed using the IP plus simvastatin combination (PFS: HR, 1.15 [95% CI, 0.56 to 2.35]; p=0.709; OS: HR, 1.61 [95% CI, 0.80 to 3.25]; p=0.187).
4. Serum lipid and lipoprotein levels
Serum lipid and lipoprotein levels were measured at baseline in 125 patients (100%) and after the 1st cycle of treatment in 111 patients (88.8%). Pretreatment levels of the serum lipids and lipoproteins were similar between the two treatment groups (Table 3). The serum LDL-C level was significantly reduced after the first cycle of treatment in the simvastatin group than in the control group (−27% vs. 7.0%, p < 0.001) (Table 3). Triglyceride (−20% vs. −6%, p=0.460) and HDL-C (5% vs. 11%, p=0.266) levels were not affected by the simvastatin treatment. Baseline increased level of triglycerides had a trend of better PFS (HR, 0.50; 95% CI, 0.23 to 1.11; p=0.089) and OS (HR, 0.58; 95% CI, 0.28 to 1.24; p=0.161), while the LDL-C and HDL-C levels were not associated with the survival outcomes (S4 Table).

The effect of simvastatin on serum lipid and lipoprotein levels
Survival improvement with IP plus simvastatin was not observed in patients with high baseline LDL-C levels or patients whose LDL-C level was significantly decreased after the 1st cycle of treatment (S3 Table).
5. Hypertriglyceridemia and survival
At the baseline, mean triglyceride concentration was 138.8 mg/dL (standard deviation, 79.6), and hypertriglyceridemia (> 200 mg/dL) was observed in 12% of the patients with ED-SCLC. Baseline hypertriglyceridemia was significantly associated with high body weight, BMI, low HDL-C level, and neutrophil-to-lymphocyte ratio (S5 Table). However, it was not associated with the ECOG performance status, smoking pack-years, liver metastasis, or serum LDH levels.
Analysis of the 1-year survival rate showed that the baseline serum LDH, liver metastasis, and triglyceride levels were significantly related to the 1-year survival rate (Fig. 3). Patients with triglyceride levels > 200 mg/dL (n=15) had 80.0% 1-year survival rate, while those with triglyceride levels ≤ 200 mg/dL (n=110) had 52.7% (p=0.046) (S6 Table). In the logistic regression model with covariates including LDH level and liver metastasis, the baseline triglyceride level remained an independent predictor for the 1-year survival rate (odd ratio, 0.23; 95% CI, 0.06 to 0.92; p=0.036).
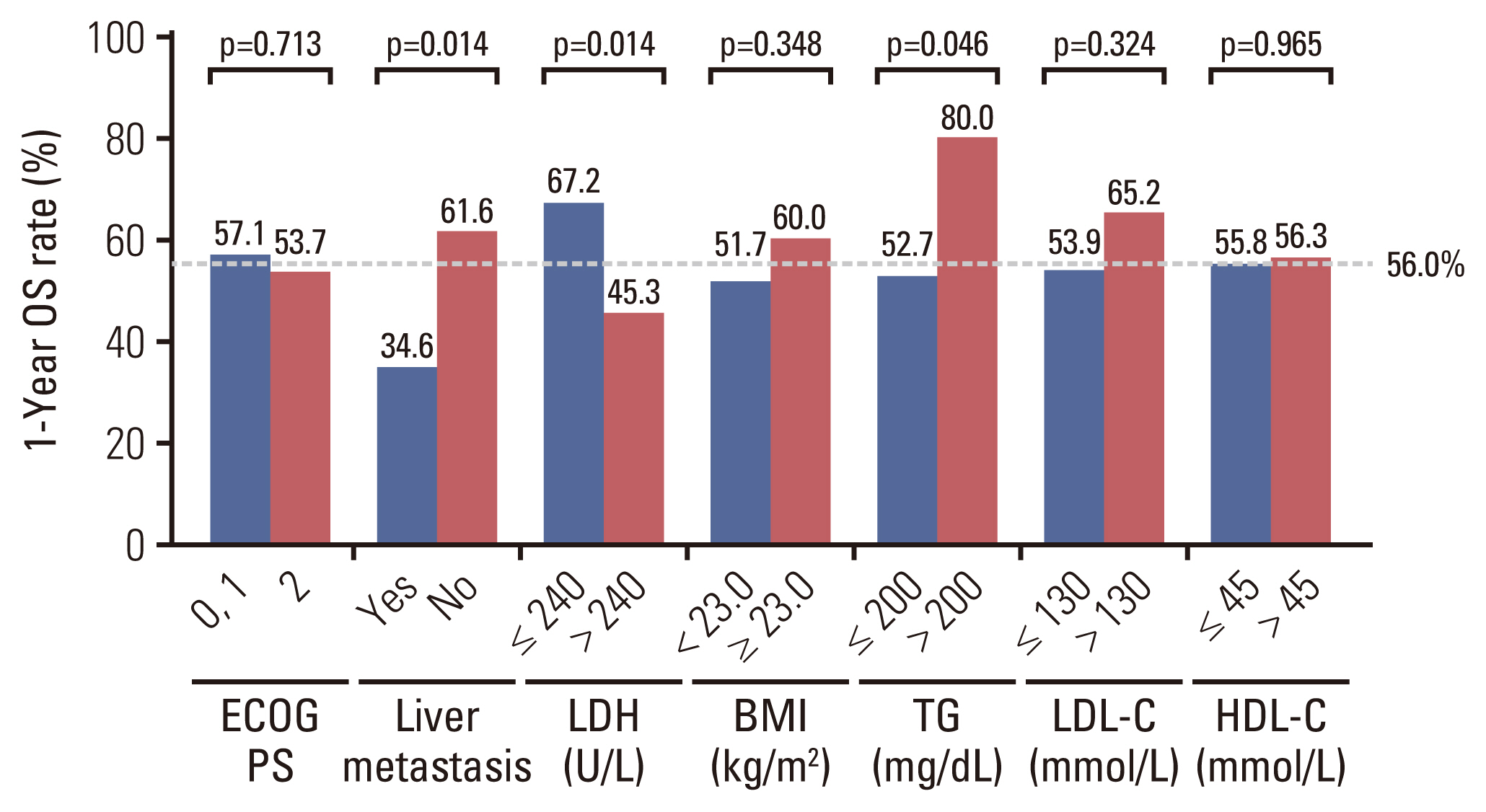
1-Year survival rate analysis by clinical factors and lipid and lipoprotein levels. BMI, body mass index; ECOG PS, Eastern Cooperative Oncology Group performance status; HDL-C, high-density lipoprotein–cholesterol; LDH, lactate dehydrogenase; LDL-C, low-density lipoprotein–cholesterol; OS, overall survival; TG, triglyceride.
Discussion
We conducted a randomized phase II study to evaluate the efficacy and toxicity of a combination of simvastatin and IP chemotherapy in 125 Korean patients with previously untreated ED-SCLC. It took almost 10 years to complete this study due to the slow recruitment. It was thought that the subject recruitment had been challenging owing to a decrease in the incidence of SCLC type and poor performance status of ED-SCLC patients [13]. In this study, IP plus simvastatin treatment failed to improve the 1-year survival rate compared to IP treatment alone. There were no significant differences in the other survival outcomes between the two treatment groups. Considering the safety profile, no additional adverse effects from simvastatin combination treatment were observed.
Based on the promising preclinical efficacy and proven safety profiles, multiple clinical studies have been conducted to investigate the anti-tumor effect of statins in different types of cancers. However, it remains controversial whether statin treatment enhances anti-tumor efficacy. In a randomized phase III study with 846 patients with ED-SCLC or limited-disease SCLC, a combination of pravastatin 40 mg/day plus standard chemotherapy did not improve the median OS compared to chemotherapy alone [14]. In addition, the sorafenib plus pravastatin 40 mg/day combination treatment showed no survival benefit in a randomized phase III study with 312 patients with advanced hepatocellular carcinoma (HCC) [15]. However, another phase II study in 83 patients with unresectable HCC demonstrated that the combination of pravastatin 40 mg/day and transcatheter arterial embolization significantly prolonged the survival [16]. Moreover, in a randomized phase II study in 91 patients with refractory multiple myeloma, lovastatin (0.5–2 mg/kg/day) combination treatment significantly prolonged the OS and PFS [17]. When statins were clinically evaluated as anticancer drugs, the type, dose, and treatment duration of statins were considered important factors affecting the final results. In this study, simvastatin 40 mg once a day treatment sufficiently lowered the mean LDL-C level by approximately 30%. However, some researchers have suggested that simvastatin 40 mg/day, which is a typical dose for hypercholesterolemia, may be a suboptimal dose to induce cancer cell death in the tissue [4]. Several doses and dosing schedules of statins need to be further evaluated in clinical settings.
In our previous clinical study, we found that the anti-tumor effect of simvastatin was associated with an increased smoking dose in patients with SCLC [11]. It was assumed that simvastatin successfully inhibited the activation of nuclear factor-κB, which plays a critical role in smoke-associated inflammatory cancers such as SCLC [18]. However, in this randomized study, the efficacy of simvastatin did not vary based on the current smoking status or pack-years. In addition, we could not find other clinical biomarkers, including BMI and lipoprotein levels, to identify cancers vulnerable to statins. In contrast, several previous studies have attempted to identify tumor subtypes with high sensitivity to statins. In a breast cancer study, the statin sensitivity of estrogen receptor (ER)–negative breast cancer was higher than that of ER-positive breast cancer [19]. Moreover, some preclinical studies showed statins are more effective in cancer cells having epithelial-to-mesenchymal transition feature [20]. HMG-CoA reductase expression or TP53 mutation status also were evaluated as a predictive molecular biomarker for statin sensitivity. However, these biomarkers have not yet been validated in clinical studies. The absence of a proven biomarker may be a cause of inconsistency in the results of many previous clinical studies with statins. Further study of predictive markers of statin-sensitive tumor type is warranted.
Although there was no significant difference in the median OS between the simvastatin and IP groups, all the patients showed an outstanding OS of approximately 15 months. This survival result appears to be distinctly longer than the historical outcomes of patients with ED-SCLC, even though this is not a direct comparison. In the IMPower133 trials, which provided the evidence of the current standard first-line treatment with atezolizumab plus etoposide and carboplatin (ECb) in patients with ED-SCLC, the median OS of the experimental and the control groups was 12.3 and 10.3 months, respectively [21]. It remains unclear why the participants of this study have a longer survival compared to that of other study controls. Several factors, including the regimen (IP vs. ECb) and treatment duration (6 cycles vs. 4 cycles) of cytotoxic chemotherapy, ethnicity (Asian vs. non-Asian), and extent of tumor could explain this unexpected result.
One of the exploratory findings of this study is the possible association between the blood lipid profile and prognosis of patients with ED-SCLC. Increased triglyceride levels at baseline were associated with better survival outcomes, independent of the LDH level, which is a well-known prognostic marker of SCLC. Few clinical studies have evaluated the prognostic effect of triglyceride; thus, the results remain inconsistent [22,23]. More recently, BMI, which is closely related to serum triglyceride levels, has been extensively investigated for its impact on the prognosis of patients treated with anti–programmed death-ligand 1 (PD-L1) immune checkpoint inhibitors in multiple cancer types [24–26]. Most previous studies have suggested that obese patients show better survival outcomes with immunotherapy than non-obese patients. Unfortunately, considering that serum triglyceride levels were not measured in those studies, we could not determine their prognostic effect in patients treated with anti–PD-L1 immunotherapy. On the other hand, cancer cachexia, which is characterized by anorexia, weight loss, and reduced skeletal muscle mass, is well known to be associated with a worse prognosis in patients with SCLC [27,28]. Impaired glucose and lipid homeostasis, such as insulin resistance, lipolysis, and systemic inflammatory process, has been suggested as a pathogenic mechanism of cancer cachexia [29]. Jones et al. [30] found that serum triglyceride levels were significantly lower in cachexic mice with tumors than in control mice owing to decreased very-low-density-lipoprotein production and release from the liver. In addition, another preclinical study reported reduced plasma triglyceride levels along with changes in the activity of tissue lipoprotein lipase in a cachexia mouse model [31]. In this study, patients without hypertriglyceridemia showed significantly lower body weight and BMI than those with hypertriglyceridemia. These findings suggest that the prognostic effect of blood triglyceride levels in patients with SCLC may be explained in terms of the cachectic conditions. However, the number of patients included in this study was too small to draw the conclusion. It is necessary to validate its prognostic value in other large-sample clinical studies.
In conclusion, the addition of simvastatin to chemotherapy provided no survival benefit in ever-smokers with ED-SCLC. Different treatment doses and schedules may be considered for increasing the synergistic anticancer efficacy. Moreover, it is necessary to evaluate whether particular SCLC subgroups are highly sensitive to statins. Among the serum lipid and lipoprotein markers, triglyceride levels could be associated with a better prognosis in ED-SCLC.
Electronic Supplementary Material
Supplementary materials are available at Cancer Research and Treatment website (https://www.e-crt.org).
Notes
Ethical Statement
This study was approved by the institutional review board of the National Cancer Center (IRB No. NCCCTS-11-527). Written informed consent was obtained from all the patients.
Author Contributions
Conceived and designed the analysis: Lee Y, Han JY.
Collected the data: Lee Y, Han JY.
Contributed data or analysis tools: Lee Y, Lee SH, Lee GK, Lim EJ, Han JY.
Performed the analysis: Lee Y, Han JY.
Wrote the paper: Lee Y, Han JY.
Administrative, Technical, or material support: Lim EJ.
Study supervision: Han JY.
Conflicts of Interest
Lee Y: Consulting fee: Roche, Merck, Yuhan, Bayer.
Han JY: Research grants: Roche, ONO, Pfizer and Takeda; Consulting fee: Astra Zeneca, BMS, Eli Lilly, Merck, Novartis, Pfizer, Abion, Jints Bio; Honoraria for lecture: Yuhan, Astra Zeneca, Pfizer, Merck, Takeda and Novartis.
Other authors have stated that they have no conflicts of interest.
Acknowledgments
We thank the patients and their families who participated in the study. This study was funded by National Cancer Center Research Grant (2210551-1). Simvastatin was supported by HK inno.N Corp.