Diagnostic Performance of Endosonography to Detect Mediastinal Lymph Node Metastasis in Patients with Radiological N1 Non–Small Cell Lung Cancer
Article information

Abstract
Purpose
Guidelines recommend that non–small cell lung cancer (NSCLC) patients with suspected hilar lymph node (LN) metastases should undergo invasive mediastinal LN staging prior to surgical treatment via endosonography. We evaluated the diagnostic performance of endosonography for detecting occult mediastinal metastases (OMM) and determined the factors associated with OMM in NSCLC patients with radiological N1.
Materials and Methods
Patients with confirmed primary NSCLC with radiological N1 who underwent endosonography for nodal staging assessment from January 2013 to December 2019 were retrospectively analyzed.
Results
The prevalence of OMM was found to be 83/279 (29.7%) and only 38.6% (32/83) were diagnosed via endosonography. However, five of them were confirmed as N3 by endosonography. The overall diagnostic sensitivity, negative predictive value, accuracy, and area under the curve of endosonography were 38.6%, 79.4%, 81.7%, and 0.69, respectively. In multivariable analysis, central tumor (adjusted odds ratio [aOR], 2.05; 95% confidence interval [CI], 1.15 to 3.68; p=0.016), solid tumor (aOR, 10.24; 95% CI, 1.32 to 79.49; p=0.026), and adenocarcinoma (aOR, 3.01; 95% CI, 1.63 to 5.55; p < 0.001) were related to OMM in radiological N1 NSCLC patients.
Conclusion
Although the sensitivity of endosonography for detecting OMM was only 40%, the prevalence of OMM was not low (30%) and some cases even turned out to be N3 diseases. Clinicians should be aware that OMM may be more likely in patients with central, solid, and adenocarcinomatous tumor when performing nodal staging in radiological N1 NSCLC via endosonography.
Introduction
Staging of non–small cell lung cancer (NSCLC) includes a variety of imaging techniques, endoscopic procedures, and surgical techniques [1,2]. Accurate staging of mediastinal lymph nodes (MLNs) is important for guiding patients to the appropriate treatment for each stage. In cases without distant metastases, NSCLC patients with no lymph node (LN) metastases (N0) or ipsilateral hilar LN metastases (N1) are usually recommended to undergo surgical resection. In contrast, patients with ipsilateral MLN (N2) or contralateral hilar/MLN metastases (N3) are referred to treatment with chemoradiation [3].
Endobronchial ultrasound–guided transbronchial needle aspiration (EBUS-TBNA) and/or endoscopic ultrasound with bronchoscope fine needle aspiration (EUS-B-FNA) are minimally invasive techniques that allow nodal staging under real-time ultrasonic guidance. They can access MLNs as well as hilar, interlobar, and lobar LNs that cannot be accessed by mediastinoscopy [4,5]. Previous studies demonstrated that endosonography (EBUS-TBNA/EUS-B-FNA) has a similar or superior diagnostic performance to mediastinoscopy in mediastinal staging [6–8]. Moreover, endosonography is the technique of choice for preoperative staging of invasive MLN according to several guidelines [1,2]. Patients with suspected hilar LN metastases are advised to undergo invasive mediastinal staging before surgical treatment [1,2]. However, evidence that endosonography accurately identifies occult mediastinal metastases (OMM) is insufficient. Studies exploring whether endosonography detects OMM in radiological N1 NSCLC to date include only a small number of patients or simultaneously evaluated radiological N0 and N1 [9,10]. In addition, information about clinical risk factors related to OMM in patients with radiological N1 NSCLC is scarce.
Therefore, in this study we aimed to evaluate the diagnostic performance of endosonography for detecting OMM and identified risk factors associated with OMM in radiological N1 NSCLC patients.
Materials and Methods
1. Study patients
This was a retrospective analysis of a prospectively collected database comprising patients with confirmed primary NSCLC with radiological N1 who underwent endosonography for nodal staging assessment from January 2013 to December 2019 at Samsung Medical Center, a tertiary referral center in the Republic of Korea.
The nodal stage inferred by computed tomography (CT) and positron emission tomography integrated with CT (PET-CT) was defined as the radiological stage, and the nodal staging determined as a result of endosonography was defined as the endosonographic stage. Radiological N1 was defined as enlarged LN on CT scan (short axis of node > 10 mm) or visual 18F-fluorodeoxyglucose (FDG) uptake on PET-CT scan in a N1 region, but neither in N2 nor N3 regions. The FDG uptake within the LN was compared with the background of the surrounding mediastinal or lung tissue and reported positive whenever an FDG uptake was higher than the background uptake [9,11]. Patients with active malignancies of other organs at the time of endosonographic diagnosis were excluded. All tumors were staged using the 8th edition of the American Joint Committee on Cancer TNM staging system [12]. All LNs were categorized into groups according to their station on the International Association for the Study of Lung Cancer LN map [13]. Central tumor was defined as a tumor located in the inner one-third of the hemithorax adopted by drawing concentric lines from the midline [14].
2. Procedure
Endosonography procedures were performed by trained physicians using a convex probe-EBUS bronchoscope (BF-UC260F-OL8, Olympus, Tokyo, Japan) and a dedicated 22-gauge needle (NA-201SX-4022, Olympus) [15]. The patients were placed under moderate sedation with intravenous midazolam and fentanyl [6]. After systematic inspection of mediastinal, hilar, and interlobar LNs, nodal sampling was performed from N3 to N2, then to N1 when the short diameter of the LN was 5 mm or more in sonography [11,16,17]. EUS-B-FNA was performed in the selected cases of station 5, 8, 9 or deeply located stations 4L, 7. We conducted three passes per node when possible. When core tissue was obtained, at least two passes were conducted whenever possible. However, when we obtained enough core tissue at the first pass and the patient’s condition was unstable, we completed the procedure after the first pass [15]. During the study period, rapid on-site cytology and elastography were not available.
For patients with no metastases to MLN and no contraindications to surgery, lung resection surgery with MLN dissection (MLND) was actively considered. MLND featured en bloc resection of all visible and palpable LNs in the ipsilateral hilum and mediastinum, irrespective of diameter (stations 10R, 9, 8, 7, 4R, 3, and 2R for right-sided tumors and stations 10L, 9, 8, 7, 6, 5 and 4 L for left-sided tumors) [11,18].
3. Diagnostic standards
Experienced pathologists analyzed all specimens sent for histological examination. Malignancy was reported based on the presence of malignant cells or cells highly suspicious of malignancy. Benignancy was reported based on the absence of tumor cells on a background of lymphoid tissue. Samples showing only blood, mucus, benign bronchial epithelial cells, or lacking lymphoid tissue were classified as inadequate and non-diagnostic [15]. The gold standard definition of OMM is the detection of MLNs metastases in either MLND or endosonographic biopsy in patients with no radiologic evidence of MLN metastases [14]. Therefore, patients who did not undergo MLND after negative results of endosonographic biopsies were not included when calculating the diagnostic performances of endosonography and evaluating the risk factors of OMM in radiological N1 disease.
4. Statistical analyses
All data are reported as the number (%) for categorical variables and as the median (interquartile range [IQR]) or mean (standard deviation) for continuous variables. Data were compared by the Mann-Whitney U test for continuous variables and the chi-square or Fisher’s exact test for categorical variables.
The diagnostic sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), accuracy, and area under the receiver operating curve (AUC ROC) of endosonography for detecting MLN metastases were analyzed. A multivariable logistic regression analysis with backward stepwise selection (with p < 0.05 for entry and p > 0.10 for removal of variables) was used to evaluate risk factors related to MLN metastases. In addition, subgroup analyses were performed to evaluate the diagnostic performance of endosonography for variables identified as risk factors for MLN metastasis through multivariable analysis. p-values < 0.05 were considered to indicate statistical significance. All statistical analyses were conducted using IBM SPSS Statistics ver. 27.0 (IBM Corp., Armonk, NY).
Results
1. Baseline characteristics
Of the 7,880 patients who underwent endosonography during the study period, 315 consecutive patients who underwent staging endosonography of radiological N1 NSCLC were included (Fig. 1). Of these, 258 patients (81.9%) underwent EBUS-TBNA only, and 57 patients (18.1%) underwent EBUS-TBNA/EUS-B-FNA concurrently. As shown in Table 1, the median age was 66 years (IQR, 60 to 73), and most patients (74.3%) were male. The median diameter of the primary tumor was 37 mm (IQR, 27 to 49), and 53.3% of tumors were centrally located. The most common histological type was adenocarcinoma (57.8%), followed by squamous cell carcinoma (38.7%).

Flowchart of the study population. CT, computed tomography; eN, endosonographic nodal stage; MLNs, mediastinal lymph nodes; MLND, mediastinal lymph node dissection; NSCLC, non–small cell lung cancer; PET-CT, positron emission tomography integrated with computed tomography; pN, pathologic nodal stage.
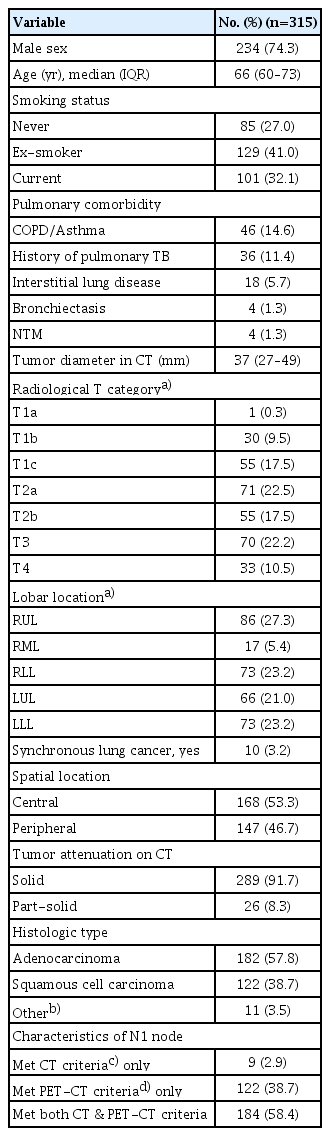
Baseline characteristics of NSCLC patients with radiological N1 disease
A total of 806 LNs were endosonographically sampled (mean, 2.6 LNs per patient) in 315 patients (S1 Table). The mean number of needle aspirations per LN was 1.7, and the mean number of core tissue samples obtained per LNs was 1.4 during a mean procedural time of 16.5 minutes. The most frequently sampled station was station 7 (the subcarinal LN, n=248), followed by station 4R (the right lower paratracheal LN, n=215) (S2 Table). EUS-B-FNA was commonly used to sample stations 4L (the left lower paratracheal LN, n=49) and 7 (the subcarinal LN, n=6).
2. Diagnostic performance of endosonography
Of 315 patients, 32 patients (10.2%) were diagnosed with OMM via endosonography (Fig. 1). Of these 32 patients, five were positive for N3 LN (primary tumor in left upper lobe and station 4R(+)=4, primary tumor in right upper lobe and station 4L(+)=1). Of the remaining 283 patients, 247 (87.3%) proceeded to surgical treatment with MLND. Of the 247 patients who underwent MLND, 51 patients (20.6%) were additionally diagnosed with pathologic N2. Eventually, after excluding 36 patients who did not receive MLND, 29.7% (83/279) were diagnosed with OMM in radiological N1 disease, and only 32 (32/83, 38.6%) patients were diagnosed with OMM via endosonography.
Patients who finally underwent MLND (n=247) and 32 patients with confirmed MLN metastases by endosonography were evaluated for the diagnostic performance of endosonography (Table 2). Using pathological confirmation as the gold standard the sensitivity was only 38.6% (95% confidence interval [CI], 28.1 to 49.9) for detecting OMM. The specificity, PPV, NPV, accuracy, and AUC ROC of endosonography were 100.0% (95% CI, 98.1 to 100.0), 100.0%, 79.4% (95% CI, 76.4 to 82.0), 81.7% (95% CI, 76.7 to 86.1), and 0.69 (0.62 to 0.77), respectively. Furthermore, of 51 patients with false-negative results for endosonography, 41 patients (80.4%) had metastases in accessible LNs via EBUS-TBNA (S3 Table). False-negative results by endosonography were most common for station 7 (n=24), followed by station 5 (n=17) and station 4R (n=11).
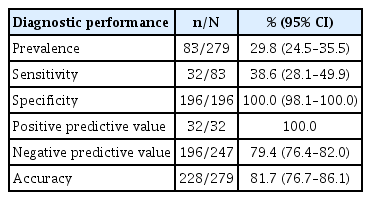
Diagnostic performance for detecting mediastinal metastases by endosonography in patients with clinical N1 NSCLC (n=279)
3. Factors associated with MLN metastases
Factors associated with MLN metastases were explored in 279 patients; patients with N0/N1 after endosonography who underwent surgical resection with MLND (n=247), and patients with N2/N3 after endosonography (n=32) (Table 3). In multivariable analysis, central tumor (adjusted odds ratio [aOR], 2.05; 95% CI, 1.15 to 3.68; p=0.016), solid tumor (aOR, 10.24; 95% CI, 1.32 to 79.49; p=0.026), and adenocarcinoma (aOR, 3.01; 95% CI, 1.63 to 5.55; p < 0.001) were related to OMM in radiological N1 NSCLC patients. In addition, the average number of sampled MLNs per patient were not statistically different between patients with true-negative (pN0/1=196; 2.1±1.0), false-negative (endosonographic N0/1 but pN2=51; 2.0±0.9), and true-positive (endosonographic N2/3=32; 2.0±0.9; p=0.840) results.

Factors related to mediastinal metastases (n=279)
Table 4 shows the results of subgroup analyses for diagnostic performance of endosonography in patients with radiological N1 according to tumor centrality, attenuation, and histology. Although patients with central, solid, and adenocarcinomatous tumor had a higher prevalence of OMM, sensitivities of endosonography for detecting OMM were not different from patients with peripheral, part-solid, and non-adenocarinomatous tumor, respectively. In accordance with the higher prevalence of OMM in patients with central or solid tumors, the NPV and accuracy of endosonography were lower in them compared with patients with peripheral or part-solid tumors, respectively.

Diagnostic performance of endosonography in patients with radiologic N1 NSCLC according to tumor characteristics
Discussion
In our study, the prevalence of OMM was 29.8% in patients with radiological N1 NSCLC. The overall diagnostic sensitivity, NPV, accuracy, and AUC ROC of endosonography were 38.6%, 79.4%, 81.7%, and 0.69, respectively. Although the sensitivity of endosonography in detecting OMM seemed low, five out of 32 patients with OMM diagnosed by endosonography were N3. In radiological N1 NSCLC, patients with OMM were related to central tumor, solid tumor, and adenocarcinoma. This is the largest study to examine the diagnostic performance of endosonography in radiological N1 NSCLC and the first to identify risk factors related to OMM in radiological N1.
In previous studies, the prevalence of OMM in NSCLC patients with negative mediastinal involvement on CT and PET-CT varied from approximately 14% to 37% [9,18–22]. However, most of these studies included radiological N0 and N1 together. In previous studies that analyzed radiological N1 only excluding radiological N0, the prevalence of OMM ranged from approximately 26% to 37% [9,19,22]. In our study, the prevalence of OMM among radiological N1 patients selected by applying strict criteria for CT and PET-CT was 29.7%. This value is similar to those reported in previous studies.
Diagnostic sensitivity and NPV of endosonography for OMM were only 38.6% and 79.4% in our study. In a prospective multicenter study with 100 radiological N1 NSCLC patients, diagnostic sensitivity and NPV of endosonography for OMM were 38% and 81%, respectively [9]. According to the results of two meta-analyses for performance of endosonography in radiological N0/N1 NSCLC, the pooled sensitivities of 9 and 13 studies were 49% (95% CI, 41 to 56) and 49.5% (95% CI, 36.4 to 62.6), respectively (S4 Table) [10,23]. In the results of subgroup analysis conducted by dividing studies into those conducted with only radiological N0 (n=3) and other studies (radiological N0/1, n=6), the prevalence of pathologic N2/3 was lower in the subgroup with radiological N0 (43/430, 10.0%) than in others (133/716, 18.6%). However, the pooled sensitivities of endosonography were similar between the two groups (47% vs. 50%) [10]. Combining the results of previous studies and our study, endosonography may seem like unsatisfactory for detecting OMM in patients with radiological N1 as well as N0. Although the prevalence of OMM in radiological N1 is higher than in radiological N0, both radiological N1 and N0 patients have normal mediastinums, and therefore the same limitations related to examining small MLNs less than 1 cm in size and similarly low sensitivities. Furthermore, stations 7, 5, and 4R accounted for the largest proportion of MLN metastases that were missed by endosonography. Stations 7 and 4R could be accessed by endosonography, but both stations have a wide range [13], which may have influenced our results. Even in previous studies examining the diagnostic performance of endosonography in radiological N1 NSCLC, MLN metastases missed by endosonography were mainly in stations 7 and 4R [9].
Although the sensitivity of endosonography for detecting OMM in radiological N1 was as low as 40%, it cannot be said that endosonography is not useful because the prevalence of OMM is not as low as 30%. In other words, if endosonography is performed on nine patients with radiological N1, OMM can be found in one patient because the number needed to diagnose in this study was 8.7 (279/32). Above all, five out of 32 patients with OMM diagnosed by endosonography were N3. If they had been treated with upfront surgery with MLND, the diagnosis of N3 would not have been possible because MLND cannot provide pathologic confirmation for LN corresponding to N3. In our study, of 247 patients with negative OMM by endosonography, 51 patients were diagnosed with pathologic N2 by MLND. However, some of them may have been N3. Considering this point, the role of endosonography is expected in that N3 can be identified in patients with radiological N1.
In our study, patients with OMM were most likely to have central tumor, solid tumor, and adenocarcinoma. Current guidelines suggest performing endosonography for mediastinal staging of centrally located tumors in suspected or proven NSCLC patients without mediastinal or hilar involvement on CT and/or PET-CT [2]. However, even in these practice guidelines, there is no uniform definition of central tumor [24]. In our previous and present studies, tumors located in the inner one-third of the hemithorax adopted by drawing concentric lines from the midline were defined as central [14]. When this definition was applied, central tumors showed a significant relationship with OMM. Considering lymphatic drainage and skip metastasis, this definition seems to be the most anatomically appropriate [14]. Unsurprisingly, the attenuation of the primary tumor lesion also affected the present study of radiological N1 disease, and solid lesions were more often associated with OMM than part-solid lesions, as in previous studies of radiological N0 disease [25,26]. We also found that adenocarcinoma was significantly associated with OMM in multivariable analysis. It has been repeatedly reported that adenocarcinoma is associated with OMM in previous studies [9,11,27,28]. Thus, the possibility of OMM should be considered in adenocarcinoma than other histological NSCLCs. However, the sensitivities of endosonography did not differ for patients with central and peripheral tumors, solid and part-solid tumors, or adenocarcinoma and non-adenocarcinoma. Thus, we suggest that patients with central, solid, and adenocarinomatous tumor should be considered at high risk of having OMM and false-negative results in endosonography. Further study is needed to determine whether endosonography is necessary for all patients with radiological N1 NSCLC or whether there are more effective subjects.
We summarized the methodologies and sensitivities for detecting N2/3 in NSCLC patients with normal mediastinum of a total 11 original articles from two meta-analysis studies (S4 Table) [10,23]. All studies showed that the average number of sampled LNs from N2/3 stations was less than three per patient. Even six studies had fewer than two per patient. In our study, an average of 2.1 MLNs per patient was sampled because rapid on-site cytology could not be performed even though endosonography was performed under moderate sedation. However, this is also a smaller number than sampling of at least three different MLN stations, which is generally recommended in the guidelines [1,2]. Since the studies were conducted on patients with normal mediastinum, aspiration was performed on small MLNs of 5–10 mm. Therefore, we believe that aspiration may have been forced to perform in fewer than 3 MLNs per patient. Additionally, based on the fact that there was no statistical difference in the number of MLNs sampled between true-negative (2.1±1.0), false-negative (2.0±0.9), and true-positive (2.0±0.9, p=0.840) patients, there was no difference in the efforts of the operators according to the endosonography results.
Our study had several limitations. First, this is a retrospective cohort study from a referral hospital that handles many cases of EBUS-TBNA/EUS-B-FNA in the nation. This may limit the generalization of our results to other institutions. Second, due to its retrospective nature, not all patients with radiological N1 NSCLC underwent endosonography and some patients with radiological N1 NSCLC underwent upfront surgery. Additionally, some patients with negative endosonography did not undergo surgical resection with MLND. Therefore, there may be selection bias. Nevertheless, our report details the diagnostic performance of endosonography for detecting OMM in the largest number of patients with radiological N1 NSCLC so far. We also provide information on risk factors associated with OMM exclusively in patients with radiological N1 NSCLC.
In conclusion, although the sensitivity of endosonography for detecting OMM was only 40%, the prevalence of OMM was not low (30%). Even five out of 32 patients diagnosed with OMM by endosonography were identified as N3 status that could have been missed by upfront surgery with MLND. In addition, we suggest that when performing nodal staging in radiological N1 NSCLC via endosonography clinicians should be aware that the likelihood of OMM and of false-negative results could be higher in patients with central tumor, solid tumor, or adenocarcinoma.
Electronic Supplementary Material
Supplementary materials are available at Cancer Research and Treatment website (https://www.e-crt.org).
Notes
Ethical Statement
This study was approved by the Institutional Review Board of Samsung Medical Center (IRB No. SMC 2022-07-158). The requirement for informed consent from patients was waived due to the retrospective nature of this study.
Author Contributions
Conceived and designed the analysis: Cho JH, Jeong BH.
Collected the data: Kim BG, Cho JH.
Contributed data or analysis tools: Cho JH, Shin SH, Lee K, Um SW, Kim H, Kim J, Shim YM, Jeong BH.
Performed the analysis: Kim BG.
Wrote the paper: Kim BG, Cho JH, Shin SH, Jeong BH.
Supervision: Shin SH, Lee K, Um SW, Kim H, Kim J, Shim YM, Jeong BH.
Validation: Lee K, Um SW, Kim H, Kim J, Shim YM.
Conflicts of Interest
Conflict of interest relevant to this article was not reported.