The Impact of EGFR Tyrosine Kinase Inhibitor on the Natural Course of Concurrent Subsolid Nodules in Patients with Non–Small Cell Lung Cancer
Article information

Abstract
Purpose
The role of epidermal growth factor receptor–tyrosine kinase inhibitors (EGFR-TKIs) in the management of persistent subsolid nodules (SSNs) is unclear. This study aimed to investigate the impact of EGFR-TKIs on concurrent SSNs in patients with stage IV non–small cell lung cancer (NSCLC).
Materials and Methods
Patients who received an EGFR-TKI for at least 1 month for stage IV NSCLC and had concurrent SSN(s) that had existed for at least 3 months on chest computed tomography were included in this retrospective study. Size change of each nodule before and after EGFR-TKI therapies were evaluated using a cutoff value of 2 mm; increase (≥ 2 mm), decrease (≤ −2 mm), and no change (−2 mm < size change < +2 mm).
Results
A total of 77 SSNs, 51 pure ground-glass (66.2%) and 26 part-solid nodules (33.8%), were identified in 59 patients who received gefitinib (n=45) and erlotinib (n=14). Among 58 EGFR mutation analysis performed for primary lung cancer, 45 (77.6%) were EGFR mutant. The proportions of decrease group were 19.5% (15/77) on per-nodule basis and 25.4% (15/59) on per-patient basis. Four SSNs (5.2%) disappeared completely. On per-patient based multivariable analysis, EGFR exon 19 deletion positivity for primary lung cancer was associated with a decrease after initial EGFR-TKI therapy (adjusted odds ratio, 4.29; 95% confidence interval, 1.21 to 15.29; p=0.025).
Conclusion
Approximately 20% of the concurrent SSNs decreased after the initial EGFR-TKI therapy. EGFR exon 19 deletion positivity for primary lung cancer was significantly associated with the size change of concurrent SSNs.
Introduction
Pulmonary nodules have been identified more frequently since the introduction of low-dose computed tomography (CT) for lung cancer screening [1,2]. Subsolid nodules (SSNs) present a homogenous density, which is increased than the lung field but does not obscure the bronchovascular structures on a chest CT scan [3]. SSNs are classified according to their composition: pure ground-glass opacity nodule (pGGN) consists of ground-glass opacity (GGO) only, while part-solid nodules (PSNs) contain both GGO and a solid component [3].
Among newly detected SSNs, transient lesions usually disappear after 3 months of follow-up [4]. In the long-term follow-up, about 17% of persistent pGGNs and 42% of persistent PSNs grow in total size or in solid portion while about 83% of persistent pGGNs and 58% of persistent PSNs are stable without spontaneous regression or disappearance [5,6]. Persistent SSNs often represent pre-invasive or invasive malignancies [7]. The malignancy rate of PSNs is known to be much higher than that of pGGN or solid nodules [5]. SSNs have a favorable prognosis when surgically resected [8,9]. However, surgery is not always possible (i.e., multiple synchronous SSNs on different lobes of lung or poor general condition of the patient).
Several reports by our group and others have explored the relationship between SSNs and the relatively high frequency of an epidermal growth factor receptor (EGFR) mutation [10–12]. As SSNs are associated with adenocarcinoma histology and an EGFR mutation [13], EGFR tyrosine kinase inhibitors (EGFR-TKIs), which are used to treat stage IV non–small cell lung cancer (NSCLC) with a sensitizing EGFR mutation, would have a role in the treatment of SSNs as well. Nevertheless, no previous report has investigated the impact of EGFR-TKIs on the course of persistent SSNs. Therefore, in this study, we investigated the impact of EGFR-TKIs on the natural course of concurrent SSNs in patients with stage IV NSCLC.
Materials and Methods
1. Study population
This study was a retrospective study performed at Samsung Medical Center (a 1,979-bed referral hospital in Seoul, South Korea). Patients who received an EGFR-TKI for at least 1 month from January 2010 to December 2015 for stage IV NSCLC and also had concurrent SSN(s) that persisted for at least 3 months on chest CT scans before initiating EGFR-TKI therapy were included as the study population. We excluded patients who (1) had been treated with an EGFR-TKI for less than 1 month, (2) had no chest CT scans before or after EGFR-TKI therapy, and (3) had a diffuse GGO or extensive lung-to-lung metastases.
Electronic medical records were reviewed to retrieve clinical information, including the initial EGFR-TKI treatment, the additional treatment after cessation of the initial treatment, and the adverse effects (AEs). The cancer treatment regimen was determined at the discretion of the attending physician. EGFR mutations for the primary lung cancer were identified using a PNA clamp kit or the real-time polymerase chain reaction [14]. The histopathologic confirmation and EGFR mutation analysis for each SSNs could not be conducted in this study since all study subjects had stage IV NSCLC and received palliative chemotherapy. Baseline data were obtained on 30 June 2019, and the follow-up data were retrieved on 31 October 2019. All methods were carried out in accordance with relevant guidelines and regulations.
2. Measurements and outcomes
Chest CT scans were obtained with 1.25-mm section thickness for transverse images with or without contrast enhancement. Chest CT images were displayed by using a lung window setting with a center of −700 HU and a width of 1,500 HU [15]. The baseline chest CT scan in which SSNs first appeared and the chest CT scans before initiating an EGFR-TKI were compared to evaluate the persistence of the SSNs, and follow-up CTs were performed every 3 months after initiating therapy or when disease progression was clinically suspected. Two experienced chest radiologists (H.Y.L. and K.H.K.) who were unaware of the clinical results, independently measured the longest diameter of the nodule in axial, coronal, and sagittal planes of lung setting of chest CT scans and then they calculated the average value of three planes. The mean value of two radiologists’ measurement was used in the analysis.
The primary outcome was to evaluate the treatment response, either a per-nodule or a per-patient basis. Each nodule was evaluated by comparing the difference in size between the chest CT before the initiation of EGFR-TKI therapy and the last chest CT scan during EGFR-TKI therapy. Regarding the slice thickness of the CT scan, size change of each nodule was classified using a cutoff value of 2 mm. Definitions of the size changes were as follows: increase (size change ≥ 2 mm), decrease (size change ≤ −2 mm), and no change (−2 mm < size change < +2 mm). For the per-patient based analysis, when a patient with multiple SSNs had different responses for each nodule, the case was considered as a decrease group if one of the SSNs decreased in size after EGFR-TKI therapy. Subtypes of SSNs were classified as pGGN or PSN. Among the subjects who had multiple SSNs, the subtypes were classified as PSN if the subject had at least one PSN and as pGGN if the subjects had all pGGNs.
3. Statistical analysis
Data are reported as numbers with percentages in parentheses for categorical variables, and as medians with interquartile ranges (IQRs) in parentheses for continuous variables. Categorical variables were compared using Pearson’s chi-square test or Fisher exact test, and the t test was used to compare continuous variables. The treatment responses were compared using the paired t test. A multivariable logistic regression analysis with backward stepwise selection (p < 0.05 for entry of variables and p > 0.10 for removal of variables) was used to identify the independent risk factors associated with the decrease in size of SSNs. All tests were two-sided, and a p-value < 0.05 was considered significant. All analyses were performed using Stata software (ver. 14.0, Stata Corp., College Station, TX).
Results
1. Patient characteristics
The study flowchart is presented in S1 Fig. A total of 77 persistent SSNs were included in the analysis of 59 patients. Forty-five patients (76.3%) had a single SSN, whereas 14 patients (23.7%) had multiple synchronous SSNs; eight (13.6%) with only pGGNs, four (6.8%) with both pGGNs and PSNs, and two (3.4%) with only PSNs. The baseline clinical characteristics of the 59 patients according to the size change are described in Table 1. Fifteen patients (25.4%) were classified as “Decrease” group, including cases of a pure decrease in size (n=10) and a mixed response with both a decrease in size and no change (n=5). Forty-four patients (74.6%) were classified as “No change or increase” group, which included cases of no change (n=43) or an increase in size (n=1). The median age of the total subjects was 58 years old (range, 54 to 67 years), and 39 (66.1%) were female. Forty-four (74.6%) were never smokers. Nine (15.3%) were treatment-naïve for lung cancer and received an initial EGFR-TKI as first-line chemotherapy. Fifty-eight (98.3%) had undergone EGFR-TKI mutation tests, while one was treated with an EGFR-TKI without confirmation of EGFR mutation status. Forty-five (77.6%) had an EGFR mutation: 22 (37.9%) with deletion in exon 19, 17 (29.3%) with a missense mutation in exon 21 (L858R), and six (10.3%) with uncommon mutations. EGFR-TKI mutation tests were performed with specimens from the primary lesion in 35 (77.8%), metastatic lymph nodes from seven (15.6%), and other metastatic organs in three (6.7%), including the brain (n=2) and liver (n=1). Gefitinib and erlotinib were used in 45 (76.3%) and 14 (23.7%), respectively. The primary lung cancer showed partial remission in 37 (62.7%), stable disease in 11 (18.6%), and progressive disease in 11 (18.6%) for the best response during initial EGFR-TKI therapy. The median time from detecting the SSNs to initiating the EGFR-TKI was 307 days (IQR, 182 to 583), and patients received the initial EGFR-TKI for a median of 308 days (IQR, 97 to 583) with followed up of median 693 days (range, 308 to 1,132 days) after initial EGFR-TKI therapy. The frequency of EGFR exon 19 deletion was significantly higher in the decrease group than in the increase or no change group (75.0% vs. 39.4%, p=0.031).

Baseline characteristics of the study population in reaction to size grouping (n=59)
2. Nodule characteristics and changes in size after the initial EGFR-TKI therapy
The baseline radiological features of 77 SSNs and size changes after EGFR-TKI therapy are summarized in Table 2 and Fig. 1. The median size of the nodules was 7.1 mm. Fifty-one SSNs (66.2%) were pGGNs and 26 (33.8%) were PSNs. On a per-nodule basis analysis (n=77), 15 (19.5%) decreased 2 mm or more and four (5.2%) disappeared completely after EGFR-TKI therapy (Table 2, Fig. 1). However, two SSNs (2.6%) increased 2 mm or more and 60 (77.9%) had no change in size after the initial EGFR-TKI therapy.

Nodule characteristics at the initiation of the initial EGFR-TKI and changes in size after the initial EGFR-TKI (n=77)
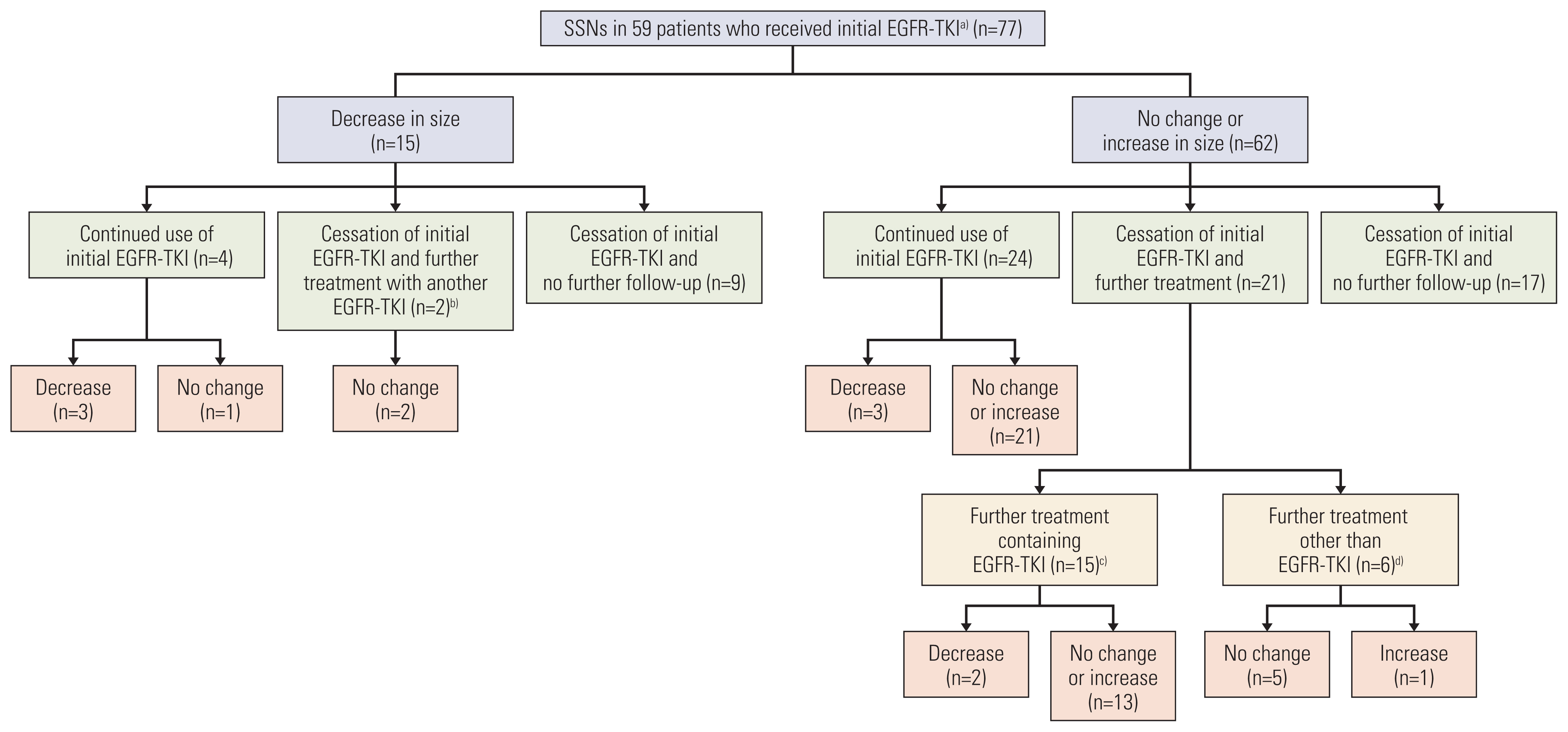
A schematic flow chart of size changes in the SSNs according to initial EGFR-TKI and subsequent therapies. EGFR-TKI, epidermal growth factor receptor–tyrosine kinase inhibitor; SSN, subsolid nodule. a)The initial EGFR-TKIs were gefitinib (n=60) and erlotinib (n=17), b)The regimens used after cessation of the initial EGFR-TKI (n=2); osimertinib (n=1) and erlotinib (n=1), c)The regimens used after cessation of the initial EGFR-TKI (n=15); afatinib (n=2), erlotinib (n=1), gefitinib (n=3), olmutinib (n=2), and osimertinib (n=7), d)The regimens used after cessation of the initial EGFR-TKI (n=6); pemetrexed/cisplatin (n=2), crizotinib (n=1), gemcitbaine/carboplatin (n=2), and vinorelbine (n=1).
Table 3 shows absolute differences in size of the SSNs in relation of the solidity of nodules and EGFR mutation status for the primary lung cancer. Among 77 SSNs, an absolute change of −0.3 mm was observed with a median pre-treatment size of 7.1 mm (range, 6.0 to 9.7 mm) and a median post-treatment size of 6.8 mm (range, 5.2 to 8.9) (p=0.001) (Table 3). The absolute change in size of pGGN and PSN between before and after initial EGFR-TKIs was −0.1 mm and −0.5 mm, respectively (p < 0.001 for pGGNs vs. p=0.182 for PSN). The absolute change in size of SSNs with EGFR mutation positivity for primary lung cancer was −0.5 mm (p < 0.001). Interestingly, the absolute difference was largest in EGFR exon 19 deletion (−1.6 mm) compared with L858R (−0.2 mm) and uncommon mutation (−0.4 mm) (Table 3). Moreover, the proportion of decrease ≤ −2 mm was highest in EGFR exon 19 deletion group (34.6%) compared with other groups (S2 Table). Fig. 2A is a representative case of a SSN showing the response to EGFR-TKIs over time.

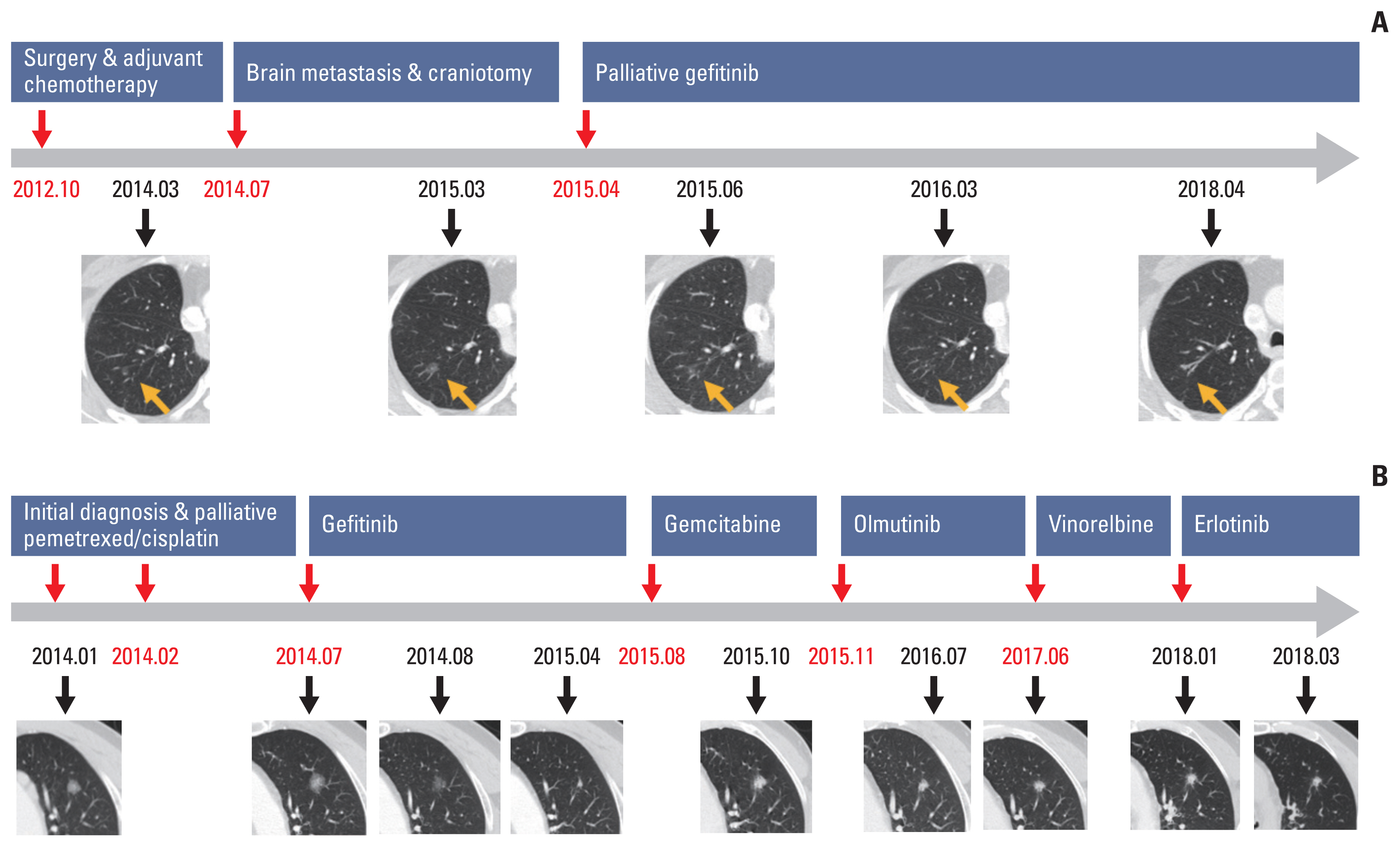
Representative cases of SSNs showing the response to EGFR-TKIs over time (A) and responding to the initial and subsequent EGFR-TKI therapies over time (B). (A) The primary tumor was positive for the EGFR L858R mutation. A pure ground-glass nodule in the right upper lobe decreased markedly in size after initiating gefitinib. (B) The primary tumor was positive for the EGFR exon 19 deletion. A part-solid nodule in the left upper lobe decreased markedly in size after initiating gefitinib. The size of the nodule increased after stopping gefitinib and initiating gemcitabine. However, the size of nodule decreased again after initiating erlotinib. EGFR, epidermal growth factor receptor; SSN, subsolid nodule; TKI, tyrosine kinase inhibitor.
3. Factors related to the decrease in size of SSNs to initial EGFR-TKI therapy
Table 4 shows the factors associated with a decrease in size of SSNs (≤ −2 mm) after the initial EGFR-TKI on per-patient based univariable and multivariable analyses (n=59). Only EGFR exon 19 deletion positivity for the primary tumor was significantly associated with the decrease in size after initial EGFR-TKI therapy (adjusted odds ratio, 4.29; 95% confidence interval, 1.21 to 15.29; p=0.025).
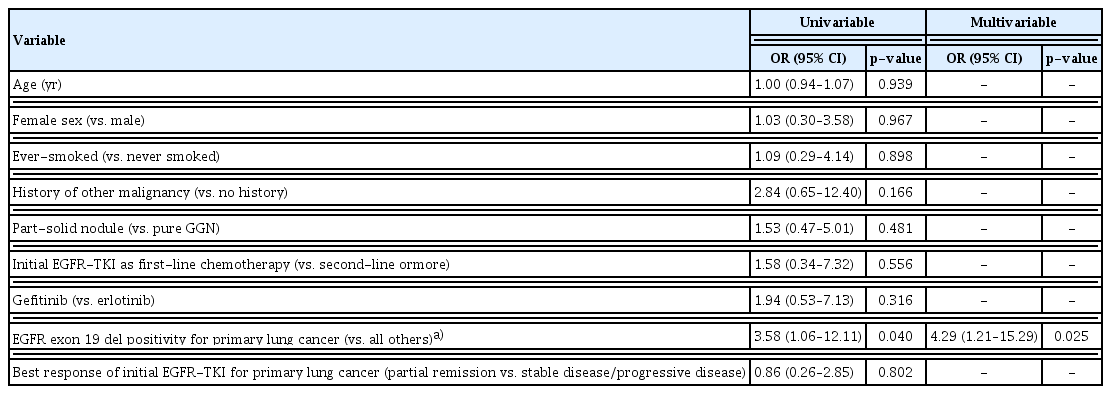
Factors associated with a decrease in SSNs (≤ −2 mm) after initial EGFR-TKI therapy on per-patient basis analysis (n=59)
4. Subsequent therapies after the initial EGFR-TKI
The study population was further followed up after cessation of the initial EGFR-TKIs and the response to subsequent therapies had been analyzed. Subsequent therapy after cessation of the initial EGFR-TKI was performed for 23 SSNs in 18 patients (Fig. 1, S3 Table). The median size of the 17 SSNs with subsequent EGFR-TKI therapy before and after the subsequent therapy was 7.9 mm (range, 5.2 to 9.7) and 5.7 mm (range, 4.8 to 8.1 mm) (p=0.374), respectively. Of the 17 SSNs with subsequent EGFR-TKI therapy, two (11.8%) decreased 2 mm or more in size when switched to a different class of EGFR-TKI with a median subsequent treatment duration of 227 days (range, 83 to 475 days) (Fig. 1). Fig. 2B shows a representative case of SSNs responding to the initial and subsequent EGFR-TKI therapies over time.
5. Adverse effects of Initial EGFR-TKI therapy
AEs (≥ grade 2) occurred in 30 patients (50.8%) who received initial EGFR-TKIs, including 21 (46.7%) in patients who were administered gefitinib and nine patients (64.3%) who took erlotinib (S4 Table). A skin rash was the most common side effect (54.2%) followed by mucositis, gastrointestinal symptoms, paronychia and abnormal liver function test. Only two (4.4%) patients had to hold gefitinib for 2 weeks due to abnormal liver function tests.
Discussion
The natural course of persistent SSNs has been of interest and is still under investigation. Although most SSNs remain stable for several years and are not aggressive, some progress eventually during long-term follow-up [5,16,17]. Persistent SSNs in Asian populations rarely decrease in size spontaneously during long-term follow-up in the previous studies [5,6]. In this study, using cutoff value of 2 mm, the proportions of decrease group were 19.5% (15/77) on per-nodule basis and 25.4% (15/59) on per-patient basis. To the best of our knowledge, this is the first study to investigate the impact of EGFR-TKI therapy on the natural course of SSNs.
The differential diagnosis of SSNs includes infection, organizing pneumonia, inflammation, focal fibrosis, atypical adenomatous hyperplasia, and neoplastic lesions (adenocarcinoma in situ/minimally invasive adenocarcinoma) [18]. Inflammatory lesion or infection usually disappear within 3 months after initial detection [4]. Persistent SSNs for 3 months or more suggest neoplastic lesions, atypical adenomatous hyperplasia, or focal fibrosis. Among 77 enrolled SSNs (51 pGGNs and 26 PSNs) in this study, 58 (75.3%) SSNs persisted more than 6 months before the initial EGFR-TKI treatment. During the follow-up from the first detection of SSNs to the initial EGFR-TKI, 36 (46.8%) increased in size and 41 (53.2%) were stable. The persistency of SSNs for a period of time prior to the initial EGFR-TKI treatment supports that they were not transient inflammatory lesion but neoplastic lesions or focal fibrosis.
Concurrent SSN(s) in a primary tumor with GGO component could either be multifocal origin or intrapulmonary metastasis, theoretically [19]. Of the 59 study subjects, the radiologic characteristics of primary tumors were solid in 47 (79.7%), part-solid in 11 (18.6%), and pure GGO in one (1.7%). In 47 subjects (79.7%) with solid-type primary tumors, concurrent SSN(s) could be regarded as an independent lesion rather than intrapulmonary metastasis from the primary tumor considering the different radiologic features. Furthermore, when we investigated the response of EGFR-TKI in 12 patients who had the primary tumor with GGO component (part solid in 11 and pure GGO in 1), the discordance rate of EGFR-TKI response between the primary tumor and SSN(s) was 66.7% (8/12). A relatively high discordant rate suggests the possibility of the multifocal origin of SSN(s) rather than intrapulmonary metastasis from the primary tumor. When we analyzed the effect of EGFR-TKI on multiple SSNs from 14 patients (2 nodules in 11 patients, 3 nodules in 2 patients, and 4 nodules in 1 patient), discordant response was observed in 50.0% (7/14). Previous studies also suggested multifocal origin of SSNs rather than intrapulmonary metastasis based on genetic studies [20,21]. International Association for the Study of Lung Cancer also proposed that T staging of multifocal SSNs should be determined by highest T lesion with either the number of tumors or m in parenthesis to denote the multifocal nature [22]. However, Li et al. [23] showed that two of multiple SSNs in two patients shared somatic mutations based on exome sequencing, indicative of intrapulmonary metastasis from tumor spread through air spaces. Since we did not perform genetic analysis of the primary tumors and SSNs in this study, it is difficult to conclude the origin of SSNs. Further in-depth genetic profiling is mandatory in the future studies to elucidate the origin of multiple SSNs.
A previous study investigated the effect of platinum-based chemotherapy on SSNs [24]. Ninety-one persistent SSNs in 51 adenocarcinoma patients received either cisplatin or carboplatin-based chemotherapy and 94.5% of the ground-glass opacity nodules (GGNs) remained unchanged in size, while 5.5% of the GGNs increased in size. No significant difference was found in the size, attenuation, volume or mass of the SSNs between baseline and post-treatment. The authors concluded that platinum-based chemotherapy may have no effect on the clinical course of persistent GGNs and explained that platinum-based agents bind and inhibit DNA replication, thus inducing cell cycle arrest which may have had a diminished effect on slowly growing SSNs. In our study, of the six SSNs that subsequently received cytotoxic chemotherapy, five (83.3%) did not change in size and one (16.7%) increased in size during follow-up (Fig. 1).
EGFR mutation positivity for primary lung cancer, especially exon 19 deletion, was significantly associated with the size change of the SSNs in this study. In the previous studies, among the subjects who were treated with EGFR-TKIs, the subjects with EGFR exon 19 deletion had more favorable clinical outcome and survival than those with L858R or other uncommon mutations [25,26]. However, pathological confirmation and genotyping of the each SSN were not performed in this study, as the study population had clinical stage IV NSCLC and were not surgical candidates. A previous work from our group showed that the EGFR mutation was detected in 88.9% of the resected SSNs using whole exome sequencing [11]. Kobayashi et al. [17] reported that EGFR mutation was noted in 64.5% of the resected SSNs using reverse transcription polymerase chain reaction in Japanese population. Li et al. [27] also showed that 50.0% of the resected SSNs harbored EGFR mutation using whole exome sequencing in Chinese population. In this study, with the exception of one patient who received an EGFR-TKI without a confirmatory mutation test due to the patient’s condition, all other study patients underwent an EGFR mutation analysis for the primary lung cancer, and approximately 80% of the patients had an EGFR mutation. Interestingly, disappearing or shrinking SSNs after EGFR-TKI therapy responded during the early phase, usually within 2–3 months after treatment initiation (Fig. 2).
Clinical follow-up with serial chest CT scans and selective surgery for the growing SSNs are the mainstay option to manage SSNs, and radiation treatment is another option for patients who are not fit for surgery [28]. However, surgery or radiation therapy is not always possible due to multiplicity, location (center of the lobes), old age, multiple comorbidities or patient refusal. In situations where surgery or radiation therapy is not feasible, we suggest that EGFR-TKIs are a potential therapeutic option for multiple growing SSNs. However, there are concerns about acquired resistance and adverse effects during EGFR-TKI therapy when utilizing EGFR-TKIs to manage SSNs. In this study, none of the SSNs initially decreased and subsequently increased during the EGFR-TKI treatment; therefore, no SSN was considered to have acquired resistance to EGFR-TKIs. Although AEs ≥ grade 2 were noticed in about 53% of cases during initial EGFR-TKI therapy, no case terminated the EGFR-TKIs due to AEs.
In previous studies, which mostly focused on the growth of SSNs, growth was defined as ≥ 2 mm [5,29]. We also use the cutoff value of 2 mm in this study. About 20% of SSNs decreased in size as a response to initial EGFR-TKI therapy and 5.2% of SSNs disappeared completely (Table 2). Therefore, EGFR-TKI seems to affect the natural course of SSNs.
Several limitations of our study should be discussed. First, it was a retrospective study conducted at a single Asian center. Racial differences must be considered, as the prevalence of EGFR mutations in NSCLC are much lower in subjects from Western countries than in those from East Asian countries [30]. Second, pathological confirmation and genotyping of the SSNs were unavailable, as the study population underwent palliative management for clinical stage IV NSCLC. Therefore, we did not compare the pathologic and genetic profile of both primary lung cancer and SSNs. Third, we did not provide data on the natural course of concurrent SSNs in patients with NSCLC who did not receive any treatment. However, based on data from previous studies about the natural course of untreated SSNs, it is possible to conclude that EGFR-TKIs affected the natural course of the SSNs. A multicenter placebo-controlled trial is needed to clarify the exact role of EGFR-TKI therapy on SSNs. The results of this study provide important background data.
In conclusion, approximately 20% of the concurrent SSNs decreased in size (≤ −2 mm) after the initial EGFR-TKI therapy. EGFR exon 19 deletion was significantly associated with the size change. EGFR-TKI therapy affected the natural course of SSNs.
Electronic Supplementary Material
Supplementary materials are available at Cancer Research and Treatment website (https://www.e-crt.org).
Notes
Ethical Statement
The Institutional Review Board of Samsung Medical Centre approved this study (IRB No. 2018-03-062-002) and waived the requirement for informed consent due to its retrospective nature.
Author Contributions
Conceived and designed the analysis: Um SW.
Collected the data: Kang N, Kim KH, Jeong BH, Lee K, Kim H, Kwon OJ, Ahn MJ, Cho J, Lee HY, Um SW.
Contributed data or analysis tools: Kang N, Kim KH, Jeong BH, Lee K, Kim H, Kwon OJ, Ahn MJ, Cho J, Lee HY, Um SW.
Performed the analysis: Kang N, Kim KH, Lee HY, Um SW.
Wrote the paper: Kang N, Lee HY, Um SW.
Conflicts of Interest
Conflict of interest relevant to this article was not reported.
Acknowledgments
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (2020R1A2C2006282 and 2019R1A4A1028268).