Extraskeletal Mesenchymal Chondrosarcoma of the Heart Responded to Systemic Chemotherapy: A Case Report
Article information
Abstract
Mesenchymal chondrosarcoma is a rare cartilaginous ne - oplasm of an extraskeletal origin, and this predominately occurs in the head and neck, and also in the lower extremities. Fewer than twenty cases of cardiac mesenchymal chondrosarcoma have so far been reported on. For the most part, the results of treatment for patients with this condition have been dismal. In this study, we describe a case of cardiac mesenchymal chondrosarcoma that responded to chemotherapy following surgical biopsy. A 46-year-old man was referred for evaluation of his pleural effusions in both lungs. Chest computed tomography revealed an ovoid-shaped mass in the posterior wall of the patient's left atrium. The echocardiogram revealed a large ovoid-shaped immobile mass (11×6 cm2) in the pericardiac space, which was attached to the posterior wall of the left atrium. Emergency pericardiostomy with closure thoracostomy was performed. Seven days later, a thoracotomy was performed for reduction and diagnosis of the cardiac mass. The pathological diagnosis was extraskeletal mesenchymal chondrosarcoma of the heart.. Postoperative chemotherapy was performed for the huge remaining mass with a combined regimen of etoposide, ifosfamide and cisplatin. After 6 cycles, the patient showed a partial response without symptoms. Although cardiac mesenchymal chondrosarcoma has been reported to be chemotherapy-resistant with a short survival duration, chemotherapy may prove to be an effective treatment modality.
INTRODUCTION
Extraskeletal chondrosarcoma is a rare neoplasm, and this is believed to represent approximately 2% of all soft tissue sarcomas (1). Furthermore, extraskeletal mesenchymal chondrosarcoma in the heart is extremely rare.
Complete resection is usually difficult. Also, the prognosis is generally quite poor as cardiac chondrosarcoma is characterized by early local recurrence and metastasis. Chemotherapy and radiotherapy are indicated for those lesions that are unsuitable for radical surgery, but the efficacy of chemotherapy and radiotherapy has not been established (1,2).
In this particular case, the patient evidenced a relatively good response to combination chemotherapy. The clinically combined symptoms were also resolved following treatment.
CASE REPORT
A 46-year-old man who suffered from chest pain and dyspnea was admitted to the emergency center. The initial simple chest x-ray evidenced pleural effusions in both lungs. On physical examination, any expiratory wheezing sounds weren't detected. However, a fraction murmur was detected, coupled with right jugular vein engorgement. His ECG was unremarkable. A chest computed tomography (CT) exam showed an ovoid mass in the posterior wall of the left atrium (LA). The echocardiogram also showed a large immobile ovoid mass (11×6 cm2) in the pericardial space, which was attached to the posterior wall of the LA, and this was accompanied by a large quantity of pericardial effusion (Fig. 1A, B).

Chest computed tomography (A) and echocardiogram (B) revealed a large ovoid immobile mass (11×6 cm2) in the pericardial space, which was attached to the posterior wall of the LA, and this was accompanied by a large quantity of pericardial effusion. Chemotherapy for six cycles was followed by chest computed topography (C) and an echocardiogram (D). The size of the immobile mass attached to the posterior wall of the LA was reduced (from 4.4×3.8 cm2 to 1.8×2.5 cm2).
Emergency pericardiostomy was immediately performed, coupled with closed thoracostomy. A pleural aspiration specimen was indicative of a cytologically malignant tumor. The extensive tumor invasion into the pericardial space rendered curative surgery impossible. Therefore, the patient underwent a biopsy of the cardiac mass in order to obtain a tissue diagnosis. The immunohistochemical studies demonstrated positivity for S-100 (chondroid differentiated cell) and CD 99 (Fig. 2).
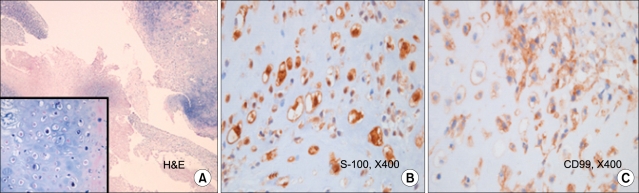
Pathologic findings of the extraskeletal mesenchymal chondrosarcoma. (A) H&E stain (B) S-100 (×400) and (C) CD99 stain (×400).
The final diagnosis was extraskeletal mesenchymal chondrosarcoma of the heart. The patient was transferred to the Hemato-oncology department for further management.
He was treated with combination chemotherapy. The regimen (VIP) consisted of etoposide (100 mg/m2, Days 1~3), ifosfamide (1500 mg/m2, Days 1~5), and cisplatin (60 mg/m2, Day 1). The cycles were repeated every 21 days.
Chemotherapy for six cycles was conducted over a six-month period, followed by chest CT, echocardiogram and positron emission tomography (PET-CT) examinations. The state of the cardiac mass with involvement of the left posterior pericardium improved, and the size of the immobile mass attached to the posterior wall of the LA was reduced (the 4.4×3.8 cm2 mass changed to 1.8×2.5 cm2) (Fig. 1C, D). The PET-CT excluded the possibility of distal metastases (Fig. 3).

PET CT showed no uptake in the cardiac mass lesion and no evidence of distant metastasis.
DISCUSSION
Extraskeletal chondrosarcoma is a rare neoplasm, and it represents approximately 2% of all soft tissue sarcomas (1). The normal age of onset is between 15 and 35 years of age, and the predominant sites of involvement include the lower limbs, head, the cranial and spinal dura matter, and the occipital portion of the neck (3). However, extraskeletal mesenchymal chondrosarcoma can also originate in the heart, although this is extremely rare.
The principal treatment for this condition is surgery. However, complete resection is usually difficult, as in our case, due to the hazardous mass in the left LA that had invaded the pericardial space. The prognosis is also generally quite poor, as cardiac chondrosarcoma is characterized by early local recurrence and metastasis. The mean survival duration is normally measured in weeks or months (4,5). Chemotherapy and radiotherapy are indicated for those lesions that are unsuitable for radical surgery, but a good result of chemotherapy and radiotherapy has not been reported (1,2).
In this particular case, the patient showed a relatively good response to combination chemotherapy. Further, the clinically combined symptoms, most notably the dyspnea and chest tightness, were resolved following treatment.
No evidence of distant metastasis was detected for distant metastasis, according to the PET-CT image evaluation. To the best of our knowledge, this is the first case of chemotherapy-sensitive extraskeletal mesenchymal chondrosarcoma of the heart. Although cardiac mesenchymal chondrosarcoma had been reported to be resistant to chemotherapy with a short survival duration, chemotherapy may prove to be an effective treatment modality.