Introduction
According to the traditional oncologic concept, local treatments for metastatic disease have very limited efficacy. Hellman and Weichselbaum first proposed the concept of “oligometastasis” in 1995, which was defined as “the intermediate status between localized and widely disseminated metastatic status” [1]. These authors later advocated the role of metastasis-directed local therapy (MDLT) based on two famous large-scale retrospective studies [2-4]. Afterwards, oncologic benefits of MDLT for oligometastatic lung cancer and prostate cancer were demonstrated by several recent randomized trials [5-7].
Approximately half of colorectal cancer (CRC) patients eventually experience metastasis to other organs [8,9], with the lung being the second most frequent metastatic site [10-12]. Since a large number of CRC patients develop distant metastasis, there is growing interest in the effectiveness of MDLT among clinicians. The first randomized trial using radiofrequency ablation for CRC patients with liver metastases, EORTC-NCRI CCSG-ALM 40004, established the role of MDLT in combination with systemic therapy [13]. The PulMiCC trial, a randomized trial that was stopped due to recruitment difficulties, failed to demonstrate the efficacy of pulmonary metastasectomy over active surveillance, thus emphasizing the limitations of surgery alone and underscoring the potential of other local treatment modality like stereotactic body ablative radiotherapy (SABR) [14]. A recent study suggested the timely performing MDLT including surgery and SABR in addition to systemic therapy could improve overall survival in CRC patients with pulmonary metastases [15]. Moreover, administration of aggressive MDLT, such as repeat SABR, might be associated with improved survival in patients with specific disease-progression patterns [16].
Although surgical resection is preferred in patients with resectable pulmonary metastatic disease [17,18], not all patients could undergo surgery due to patients’ medical comorbidities or disease status. Furthermore, probable complications associated with anesthesia and/or surgical procedures could be burdensome for these patients. With advancement of radiation therapy (RT) technologies, precise and focal delivery of high dose radiation to the target has become possible. SABR is one of the representative examples of modern RT technique that can deliver ablative high dose precisely to targets within a short period of time by applying hypofractionation. By virtue of high local tumor control rate at low level toxicity risk, SABR has emerged as an alternative local treatment option for oligometastases (OM) patients who are unable or unwilling to undergo surgery [19,20]. Favorable clinical outcomes have been reported in several studies, and there has been a recent increase of interest for the efficacy of SABR in treating CRC patients with pulmonary OM.
In CRC patients, pulmonary metastasis is one of the most common patterns of distant metastasis, and it could be detrimental to the prognosis of the patients [11]. However, if appropriate treatments for lung metastases are conducted, there is a possibility to improve the prognosis for CRC patients with pulmonary OM [12]. While there is general agreement that systemic therapy constitutes the standard of treatment for CRC patients with pulmonary OM, the current National Comprehensive Cancer Network guidelines suggest surgical resection or ablative interventions as the preferred option of MDLT for patients with amendable to cure [21]. However, there is no clear consensus in regard to the role of SABR in pulmonary OM. In this context, the purpose of this systematic review and meta-analysis was to investigate clinical efficacy of SABR in treating CRC patients with pulmonary OM and to provide integrated information for future reasonable decision-making by oncologists.
Materials and Methods
1. Information sources and searching strategy
This study was conducted according to the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement, which provided guidelines for reporting systematic reviews and meta-analyses. Methods were carefully planned and executed to ensure reliability and validity of findings [22]. To identify relevant studies, electronic databases were searched using a combination of keywords and Medical Subject Headings (MeSH) terms. Search terms were selected based on their relevance to research questions. They included terms related to primary cancer site (colorectal, colon, sigmoid, rectal, cancer, carcinoma, tumor, neoplasm), metastatic site (lung, pulmonary, metastasis), and treatment (stereotactic body radiotherapy, stereotactic radiotherapy, stereotactic ablative radiotherapy, radiosurgery, stereotactic radiosurgery, stereotactic body radiation therapy). Studies published from June 2012 to June 2022 were searched from online databases of MEDLINE and Embase using selected terms. Original articles with information about human or clinical trials and written in English were chosen. Case reports, literature review, editorial, and only abstracts were excluded from this analysis.
2. Data items and collection process
The primary endpoint of this study was overall survival (OS). Secondary endpoints included progression-free survival (PFS) and local control (LC). We used a pre-standardized sheet to acquire the following data from studies: general information including author name, year of publication, affiliation, and design of studies; clinical information including number of patient numbers, definition of OM (e.g., up to 3 or 5 metastatic foci), age, gender, tumor size, and radiation dose; treatment outcomes including rate of OS, LC, PFS, and complication of grade 3 or higher. Data acquisition and assessment were performed by two researchers (J.U.J., C.H.R.).
3. Quality assessment
Considering that majority of available literatures were observational studies, we used the Newcastle-Ottawa scale (NOS) for quality assessment [23]. Studies were classified as high-quality studies if their NOS scores were 7-9. Those with NOS scores of 5-6 were considered as medium-quality studies and those with NOS scores of 4 or less were classified as low-quality studies. Low-quality studies were excluded from this meta-analysis after reevaluation and agreement among authors.
4. Statistical analyses
The effect measure was pooled percentile of retrieved endpoints of interest (LC, PFS, and OS). Considering possible heterogeneity in clinical regards among institutions and recommendation of Cochrane Handbook regarding pooled analysis of non-randomized studies, the random effects model was used for pooled analyses. Cochrane Q test and I2 test were performed for heterogeneity evaluation and I2 statistic of 25%, 50%, or 75% indicated a low, moderate, or high heterogeneity, respectively [24,25]. Publication bias assessment was performed using visual funnel plot assessment and quantitative Egger’s test [26]. Two-tailed p-value of < 0.1 indicated a possible publication bias. The Duval and Tweedie’s trim and fill was performed as sensitivity test for analyses with possible publication bias [27]. A comparative analysis was conducted using selected studies in which LC and OS were clearly described according to the radiation dose. All statistical analyses were performed using Comprehensive Meta-Analysis ver. 3 (Biostat Inc., Englewood, NJ).
Results
1. Study selection and characteristics
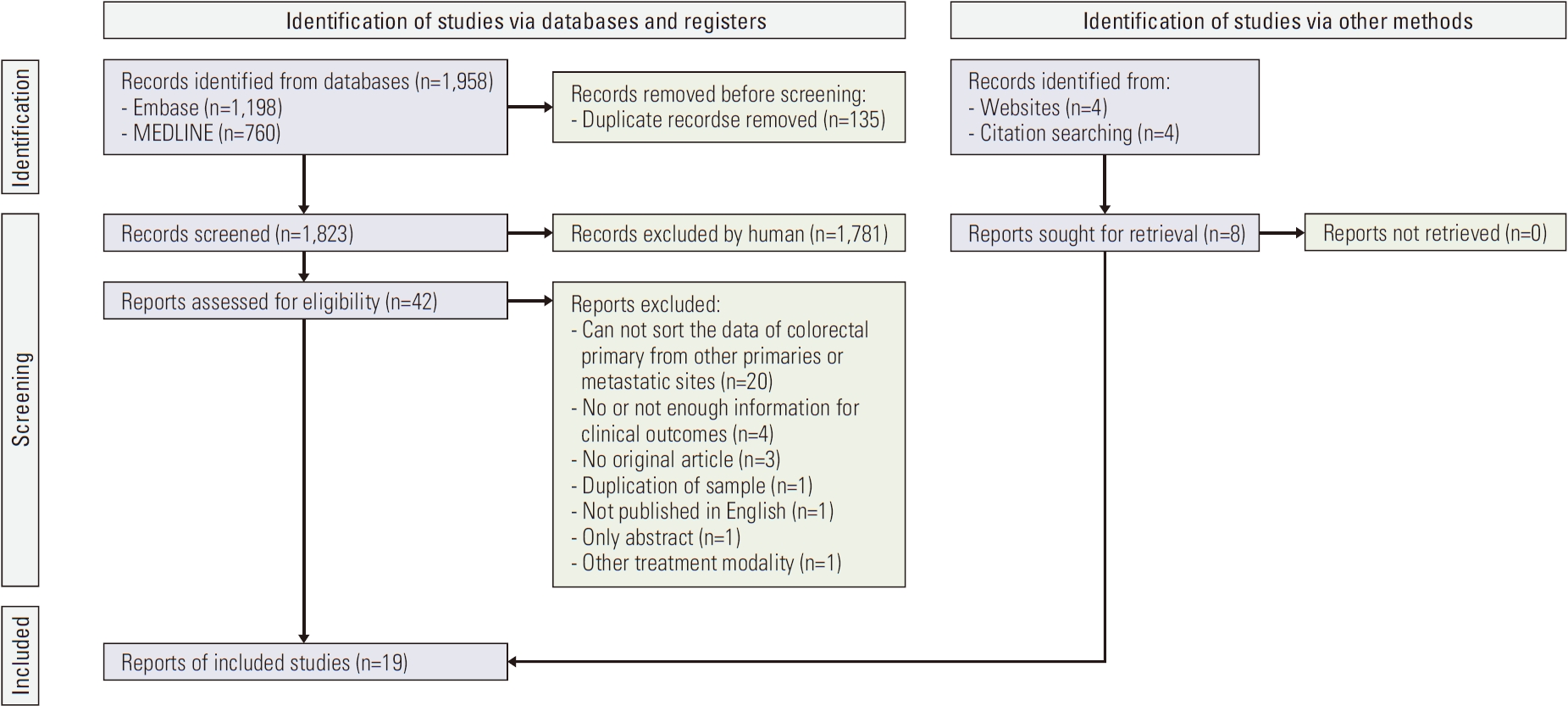
We identified 1,958 studies from the two databases: 1,198 from Embase and 760 from MEDLINE. Among these, 135 duplicated studies were removed. Remained 1,823 studies were screened and 1,781 were excluded. A total of 42 studies were selected to conduct full text review. After an eligibility evaluation process, 31 studies were excluded. Additional eight studies were identified through website search and citation tracking. They were included in the current study. Finally, a total of 19 studies with 1,668 patients were used for this meta-analysis (Fig. 1) [28-46].
Most studies included in the present analysis were retrospective studies except for two. Fourteen studies used the definition of OM by the number of lesions, while five used the maximum number of lesions. The median biologically effective dose (BED) of SABR with an α/β ratio of 10 (BED10) ranged from 93.6 Gy to 180 Gy (Table 1). Clinical outcomes from each study are shown in Table 2. Among a total of 19 studies, 16, 10, and 12 studies reported LC, PFS, and OS, respectively. The assessment for LC was based on metastatic lesions except for two studies [34,42].
2. Quality assessment
All selected studies were categorized to have a medium quality. Therefore, no study was excluded from subsequent pooled analyses. Detail sheet of scoring and reason of scoring are shown in S1 Table.
3. Synthesized results
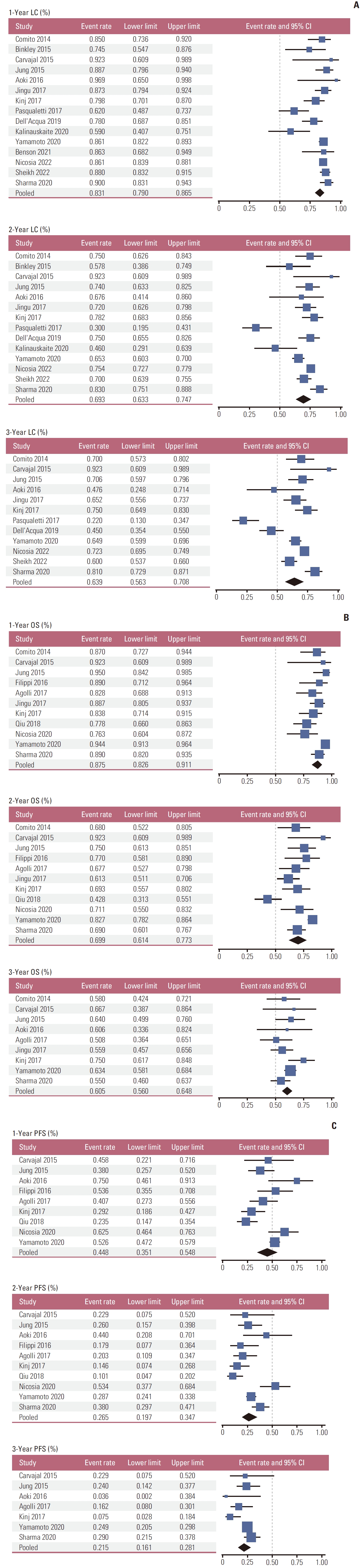
Pooled rates of LC at 1-, 2-, and 3-year were 83.1% (95% confidence interval [CI], 79.0% to 86.5%), 69.3% (95% CI, 63.3% to 74.7%), and 63.9% (95% CI, 56.3% to 70.8%), respectively (Fig. 2A). Pooled OS rates at 1-, 2-, and 3-year were 87.5% (95% CI, 82.6% to 91.1%), 69.9% (95% CI, 61.4% to 77.3%), and 60.5% (95% CI, 56.0% to 64.8%), respectively (Fig. 2B). Pooled PFS rates at 1-, 2-, and 3-year were 44.8% (95% CI, 35.1% to 54.8%), 26.5% (95% CI, 19.7% to 34.7%), and 21.5% (95% CI, 16.1% to 28.1%), respectively (Fig. 2C). Treatment-related toxicities were reported in 13 studies. Pooled complication rate of grade 3 or higher was 3.6% (95% CI, 1.9% to 6.8%) (S2 Fig.). Majority of reported grade ≥ 3 toxicities were radiation pneumonitis, while Sheikh et al. [46] reported three (2.3%) cases of bile duct stenosis. Heterogeneity assessment showed moderate to high heterogeneity in most of the pooled analyses. Synthesized results are shown in Table 3.
4. Publication bias
The publication bias assessment was performed for LC, OS, PFS, and grade ≥ 3 complication pooled analyses. Possible publication bias was not found in pooled analyses of LC, OS, or PFS. However, it was found in pooled analyses of treatment complication (Egger’s p=0.026). The Duval and Tweedie’s trim and fill was performed for pooled analysis of complication rate, which yieded an adjusted value of 5.1%. Visual funnel plots including Egger’s p-values are shown in S3 Fig.
5. Radiation dose assessment among studies
Most studies included in this meta-analysis evaluated clinical outcomes based on radiation dose. Seven studies specifically examined the effect of radiation dose on clinical outcomes (Table 4). In five out of seven studies, dose escalation was found to be a favorable factor for clinical outcomes. Four studies reported that dose escalation was a good prognostic factor for LC, while three studies found that it was beneficial for OS.
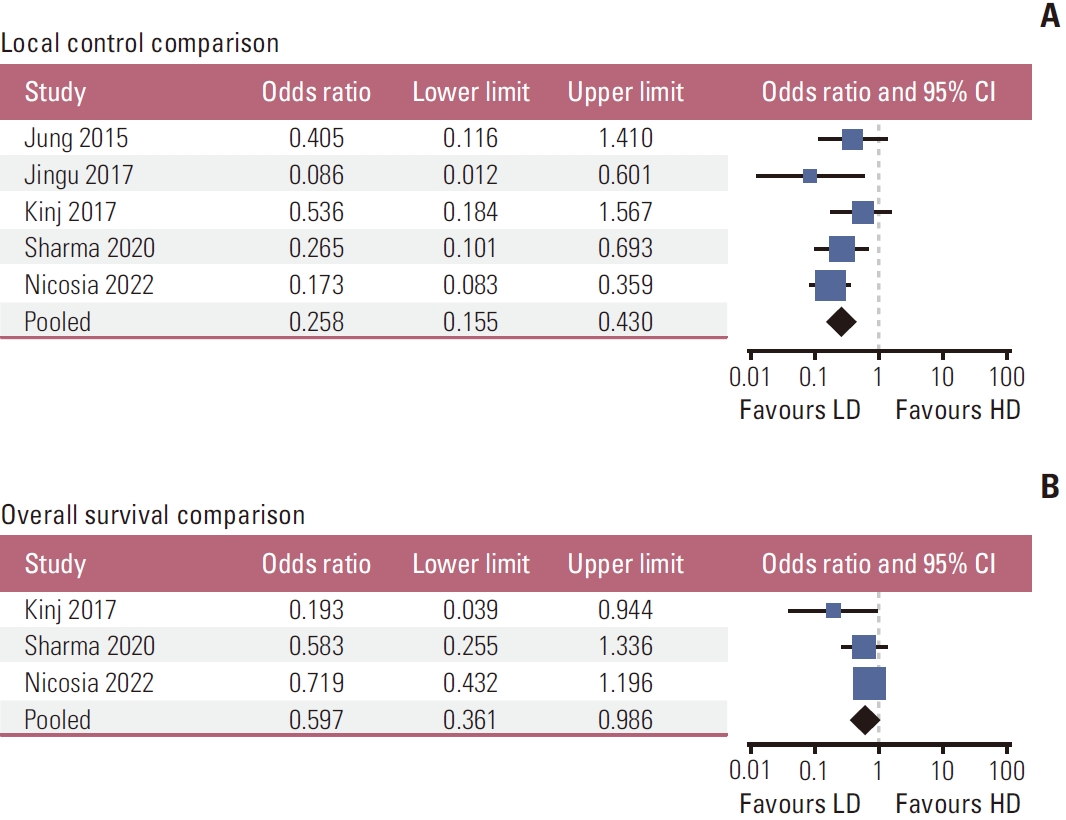
To further investigate the impact of SABR dose on treatment outcomes, we conducted a meta-analysis using data from five studies [31,35,36,42,45] on LC and three studies [36,42,45] on OS (Table 5). The analysis showed that the higher radiation-dose group (more than 100 Gy in BED10) had better LC than the lower radiation-dose group (odds ratio [OR], 0.258; 95% CI, 0.155 to 0.430; p < 0.001) (Fig. 3A). Furthermore, we found that dose escalation could lead to improved OS (OR, 0.597; 95% CI, 0.361 to 0.986; p=0.044) (Fig. 3B).
Discussion
In the current meta-analysis, pooled LC, PFS, and OS rates were 69.3%, 26.5%, 69.9% at 2-year and 63.9%, 21.5%, and 60.5% at 3-year, respectively. These results were comparable to those following pulmonary metastasectomy, with 3-year survival rates of 58% and 67.7% reported in the United States and Korea, respectively [47,48]. One study used in present analysis showed that the treatment result of SABR were not inferior to those of surgery for CRC patients with pulmonary OM [33]. For patients who are unable or unwilling to undergo surgery, SABR could be an alternative option for MDLT. This meta-analysis demonstrates that SABR could be a feasible option for CRC patients with pulmonary OM.
Therapeutic efficacy of SABR in treating pulmonary OM has been reported to be non-inferior to that of surgical resection, while SABR could lead to less frequent severe complications than surgical resection [33]. Major toxicities associated with SABR for pulmonary lesions typically include pneumonitis, chest wall pain, and neuropathy. Reported rates of toxicity vary among studies. They might have been influenced by factors such as tumor burden, location, and radiation dose [49]. While two studies reported severe toxicity rates around 10%, the majority of studies, including those included in this meta-analysis, reported no severe toxicities greater than grade 3.
There is considerable heterogeneity in the clinical characteristics among the patients included in these analyses. The number of metastases varied from 1 to 5 and the presence of extrapulmonary metastases differed among included studies. Chemotherapy before SABR was administered to the majority of patients, ranging from 58% to over 90% in each study except one. SABR was performed using either a linear accelerator or CyberKnife and it was ensured that either the percent volume receiving at least 95% of the prescription dose was over 95% or the 60%-90% isodose line of the prescribed dose covered the planning target volume. There are several points of consideration for determining the optimal dose of SABR based on the heterogeneity in clinical settings. First, various dosimetric parameters should be considered, not only prescribed radiation dose but also maximum and average dose for targets in the era of advanced radiotherapy technologies such as intensity-modulated and volumetricmodulated arc therapies, which enable more accurate dose distribution [50]. The presence of a hot spot within the tumor volume might have the potential to increase LC. Several studies included in this research have made efforts to ensure the hot dose within the tumor volume such as at least 120% of the prescription dose in gross target volume [29] or > 105% of the prescription dose within planning target volume [30]. Second, the radiobiological parameter is differed according to the primary histology and metastatic organ, and it should be taken into consideration to determine the optimal radiation dose [51]. Several studies included in the present analysis reported that colorectal histology showed worse prognosis than other types of primary tumors [29,32]. Although the treatment outcomes of SABR would be varied among CRC patients in the present study, depending on factors such as the primary tumor site (colon or rectum) [36], genetic influences (BRAF or KRAS mutations) [36,41], and metastatic sites (lung, liver, or others) [46]. However, one study reported that there was no difference in local PFS according to the primary site (colon or rectum) or genetic mutation [45]. It is still challenging to evaluate biologic effects on prognosis after SABR. Third, radiation dose to obtain the same tumor control probability may differ due to clinical factors such as tumor extent. Several studies included in this analysis also showed various prescribed doses depending on tumor size and location, and surrounding organs at risk [28,33,34,36,37,42,45,46]. It was observed that tumors with small size [28,33,34,37,45,46], small number of metastatic lesions [34,36], and peripheral tumors [34,36,37,40] tended to have an increased BED10, ranging from 120 to 180 Gy, compared to others, ranging from 75 Gy to 100 Gy. For these reasons, the ideal dose of SABR remains undetermined, but clinical efforts are needed to find the appropriate dose for each metastatic CRC patients.
Delivering optimal radiation dose by SABR could be essential to achieve tumor control probability. The appropriate dose of SABR is a crucial factor in predicting clinical outcomes. Several studies have previously shown that higher BED10 is associated with reduced local recurrence [35,42,43,45]. One study has found that local recurrence is higher in patients treated with a BED10 < 100 Gy than in those receiving > 100 Gy [29]. Other studies have reported a significant positive correlation between BED10 and LC, with cut-offs ranging from 75 Gy to 112.5 Gy [39]. Increasing the BED10 to higher than 100 Gy has been shown to be able to improve local tumor response, which could lead to an improved OS rate. For patients with pulmonary OM, the median survival time longer than 4 years could be expected following BED10 > 100 Gy, whereas it could be shorter than 3 years following BED10 < 100 Gy [42,45]. It seems appropriate administering SABR with BED10 ≥ 100 Gy for pulmonary metastatic lesions.
When applicating SABR to metastatic CRC patients, several clinical scenarios should be taken into consideration. The inherent tumor characteristics, such as metastatic tumor burden, which includes the number of metastatic lesions and tumor volume, could affect the prognosis for CRC patients with pulmonary OM. In present analysis, cases of small tumor burden in the lung showed a trend of higher prescribed BED10, ranging from 112.5 to 180 Gy, compared to those of large tumor burden, ranging from 76 to 87.5 Gy, and metastatic tumor burden was determined to be an independent factor for prognosis [29,36,38-40,42,45,46]. The prognosis might be different regarding to timing the occurrence of metastases. Metachronous onset of OM was a favorable factor for survival in a study to estimate the prognosis of oligometastatic patients [52,53]. In CRC patients with pulmonary OM, the 3-year survival rate was 73.5% with disease-free interval more than 2 years, while it was 65% in patients with disease-free interval less than 2 years [54]. In present analysis, metachronous disease showed better prognosis in LC [40] and PFS [34,38] compared to synchronous disease. Patients with slow-growing disease like metachronous tumors would benefit more from SABR and administration of subsequent treatments would be delayed [29]. A significantly large portion of metastases with CRC patients received chemotherapy prior to SABR and chemotherapy before SABR would influence tumor control rate [55]. In the present analysis, administration of chemotherapy before SABR was reported to have no effect on treatment outcomes in some studies [41,45], but many other studies showed a negative effect on prognosis [38,42-44,46]. Interestingly, one study demonstrated that adjuvant chemotherapy after SABR was a favorable factor for LC [35]. Macroscopic tumor shrinkage after chemotherapy could result in a marginal miss of microscopic disease, and surviving tumor cells after chemotherapy are likely to be more radioresistant.
However, our study has several limitations, which should be taken into consideration when interpreting our findings. First, most studies included in our meta-analysis were retrospective in nature and some studies had a small sample size, which might have led to a selection bias. Additionally, there were significant differences in treatments (chemotherapy or surgery) delivered to patients prior to SABR. It is difficult to evaluate the efficacy of SABR exactly unless factors like tumor size, treatment timing or sequence (i.e., pretreatment chemotherapy and SABR), and appropriate radiation dose is adequately controlled. Therefore, randomized trials are needed to identify eligible patients and determine the optimal SABR dose schedule in a clinical setting.
In conclusion, our meta-analysis demonstrates the potential role of SABR in treating CRC patients with pulmonary OM. Our study supports the use of SABR as a viable option for local tumor control. Several studies have shown the optimal BED10 of SABR is more than 100 Gy, but it still requires efforts to figure out ideal dose via clinical trials. Nevertheless, SABR could be a valid option in treating pulmonary OM for ineligible patients to undergo metastasectomy. Further studies with a larger sample size and randomized study design are highly desired to confirm our findings and determine the optimal treatment strategies.