A Predictive Model Based on Bi-parametric Magnetic Resonance Imaging and Clinical Parameters for Clinically Significant Prostate Cancer in the Korean Population
Article information
Abstract
Purpose
This study aimed to develop and validate a predictive model for the assessment of clinically significant prostate cancer (csPCa) in men, prior to prostate biopsies, based on bi-parametric magnetic resonance imaging (bpMRI) and clinical parameters.
Materials and Methods
We retrospectively analyzed 300 men with clinical suspicion of prostate cancer (prostate-specific antigen [PSA] ≥ 4.0 ng/mL and/or abnormal findings in a digital rectal examination), who underwent bpMRI-ultrasound fusion transperineal targeted and systematic biopsies in the same session, at a Korean university hospital. Predictive models, based on Prostate Imaging Reporting and Data Systems scores of bpMRI and clinical parameters, were developed to detect csPCa (intermediate/high grade [Gleason score ≥ 3+4]) and compared by analyzing the areas under the curves and decision curves.
Results
A predictive model defined by the combination of bpMRI and clinical parameters (age, PSA density) showed high discriminatory power (area under the curve, 0.861) and resulted in a significant net benefit on decision curve analysis. Applying a probability threshold of 7.5%, 21.6% of men could avoid unnecessary prostate biopsy, while only 1.0% of significant prostate cancers were missed.
Conclusion
This predictive model provided a reliable and measurable means of risk stratification of csPCa, with high discriminatory power and great net benefit. It could be a useful tool for clinical decision-making prior to prostate biopsies.
Introduction
Prostate-specific antigen (PSA) has been used extensively for diagnosis and risk assessment of prostate cancer (PCa) [1,2]. PSA level-based screening and risk stratification may reduce the PCa mortality risk; however, it still has limitations, due to the low specificity for distinguishing between benign and malignant disease [3]. To improve the specificity of PSA-based screening and risk stratification for PCa, several approaches using clinical parameters, biomarkers, and even genomic markers have been proposed [4–7]. Individualized pre-biopsy risk assessments using predictive models (risk calculators) based on useful predictive factors could help to improve the accuracy of risk stratification and further reduce and avoid unnecessary prostate biopsies [6]. Recently, multiparametric magnetic resonance imaging (mpMRI) has emerged as useful for the diagnosis and management of PCa, with a high sensitivity and negative-predictive value for clinically significant PCa (csPCa) [8,9], and mpMRI findings are accepted as useful for risk stratification. There have been many attempts to create accurate csPCa predictive models by combining clinical parameters, biomarkers, and imaging risk assessment based on mpMRI. These have relatively good reliability and are currently available (areas under the receiver operating characteristic [ROC] curve [AUC], 0.797 to 0.850) [10–12]. However, the use of biomarkers and genomic markers is costly and laboratory-dependent, and mpMRI is time-consuming (~40 minutes) and expensive. In contrast, bi-parametric magnetic resonance imaging (bpMRI) is rapid (~15 minutes) and simpler, while sufficiently retaining the diagnostic value of mpMRI [13]. The promising value of bpMRI for PCa diagnosis has recently been reported [14–18]. Here, we developed a reliable and easily applicable predictive model based on a combination of bpMRI and routinely obtained clinical parameters to improve the risk stratification of csPCa.
Materials and Methods
1. Patient selection for constructing the predictive model
We have already reported a protocol for transperineal bpMRI–ultrasound fusion targeted and systematic biopsy [19]. Briefly, we used bpMRI on a 3.0-T scanner (Siemens Medical System, Erlangen, Germany) and Prostate Imaging Reporting and Data Systems (PI-RADS) scores were reported by three dedicated uro-radiologists according to PI-RADS ver. 2.0. To develop the predictive model, medical records of 300 men who underwent transperineal bpMRI-ultrasound (bpMRI-US) fusion biopsy were analyzed. We developed a predictive model based on the results of the prior study.
2. Patient selection for external validation
We analyzed the medical records of an additional 148 men who underwent transperineal bpMRI-US fusion prostate biopsy after the period of the prior study, from April 2019 to February 2020. The protocol for prostate biopsy was the same as that in the prior study.
3. Statistical analysis
All potential predictors of csPCa, including age, body mass index, comorbidities (hypertension, diabetes mellitus), PSA, PSA density (PSAD), total/free PSA ratio, and PI-RADS score, were assessed for all patients. PSAD was divided into groups: < 0.07, 0.07–0.09, 0.10–0.14, 0.15–0.19, 0.20–0.24, and ≥ 0.25 ng/mL/g, and the PSAD group variable was considered as a continuous variable for all analyses. Univariate logistic regression models were used to analyze the effect of these variables on csPCa, and the results were presented as odds ratios and 95% confidence intervals (CIs). To quantify the discriminatory accuracy of each variable for identifying men with and without csPCa, ROC curve analyses were performed, and the results were summarized as the AUCs and 95% CIs. In univariate analysis, only variables with a p-value < 0.05 were included in the multiple logistic regression models. For clinical use, we developed a predictive model that estimated the probability of csPCa. The c-statistics and 95% CI were used to assess the predictive power of multivariable models. The best model, with the largest c-statistic, was presented as a nomogram for clinical application. Clinical utility was assessed via decision curve analysis, which estimate the “net benefit” by summing the benefits (true-positives biopsies) and subtracting the harms (false-positive biopsies) [20]. We used a calibration plot to explore predictive performance. Bootstrap resampling was performed for internal validation, and the Hosmer-Lemeshow test was performed for external validation. All statistical analyses were performed using SAS software ver. 9.4 (SAS Institute Inc., Cary, NC) and R software ver. 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria). A two-sided p-value < 0.05 was considered statistically significant.
Results
1. Study population for creating a predictive model
Three hundred patients formed part of the cohort for creating the predictive model; their characteristics are summarized in Table 1. The overall mean PSA and PSAD were 11.3 ng/mL and 0.33 ng/mL/g. PCas were detected in 158 of 300 men (52.7%), and the prevalence of csPCa was 34.0%. CsPCas were detected in 12 of 102 patients with PI-RADS 3 (11.8%), 42 of 92 with PI-RADS 4 (45.7%), and 45 of 62 with PI-RADS 5 (72.6%).
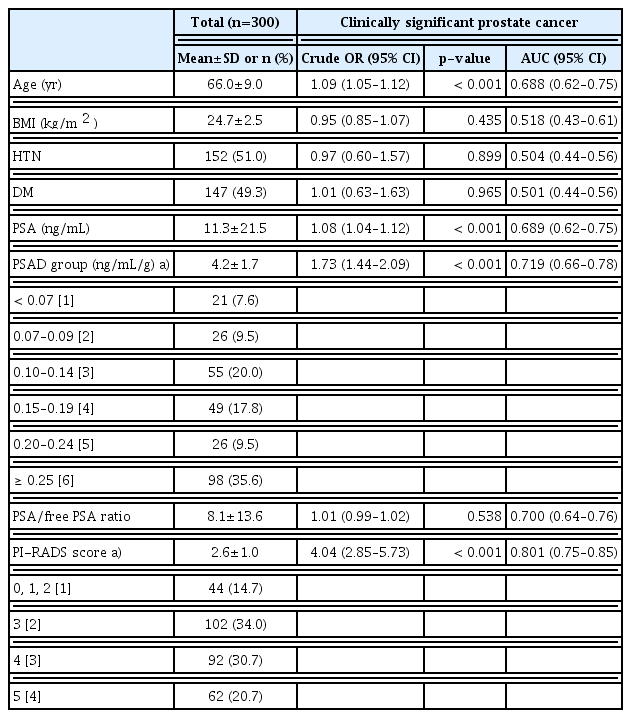
Univariate analysis of potential predictors of clinically significant prostate cancer (Gleason score ≥ 7 [3+4])
2. Study population for external validation
One hundred forty-eight patients formed part of the cohort for external validation of the predictive model. There were no significant differences among the clinical parameters and PI-RAD scores between patients. The patients’ demographic data and baseline characteristics are listed in S1 Table.
3. Development of the model for predicting csPCa
The variables age, PSA, PSAD group, and PI-RADS scores were statistically significant predictors of csPCa (p < 0.001) on logistic regression analysis. Among these predictors for csPCa, the PI-RADS scores had the highest expiratory accuracy (AUC, 0.801; 95% CI, 0.751 to 0.851) (Table 2).
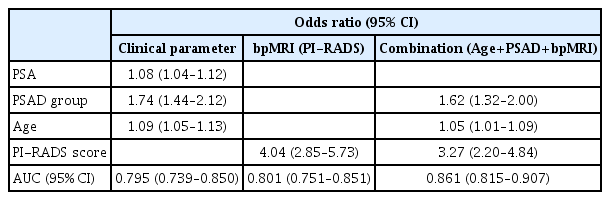
Logistic regression analysis of the multivariable models that estimate the probability of clinically significant prostate cancer at biopsy (Gleason score ≥ 7 [3+4])
In the ROC curve analysis, for the predictive model using only clinical parameters, the AUC was 0.795 (95% CI, 0.739 to 0.850). The model using only the radiologic parameter (bpMRI PI-RADS scores) yielded an AUC of 0.801 (95% CI, 0.751 to 0.851). A combined predictive model was created, and the AUC was increased to 0.861 (95% CI, 0.815 to 0.907) (Table 2).
A nomogram for predicting csPCa was developed, and an equation capable of providing estimated probability of csPCa was developed using the best multiple logistic regression model (Fig. 1): Estimated probability of csPCa=exp(lp)/[1+exp(lp)].
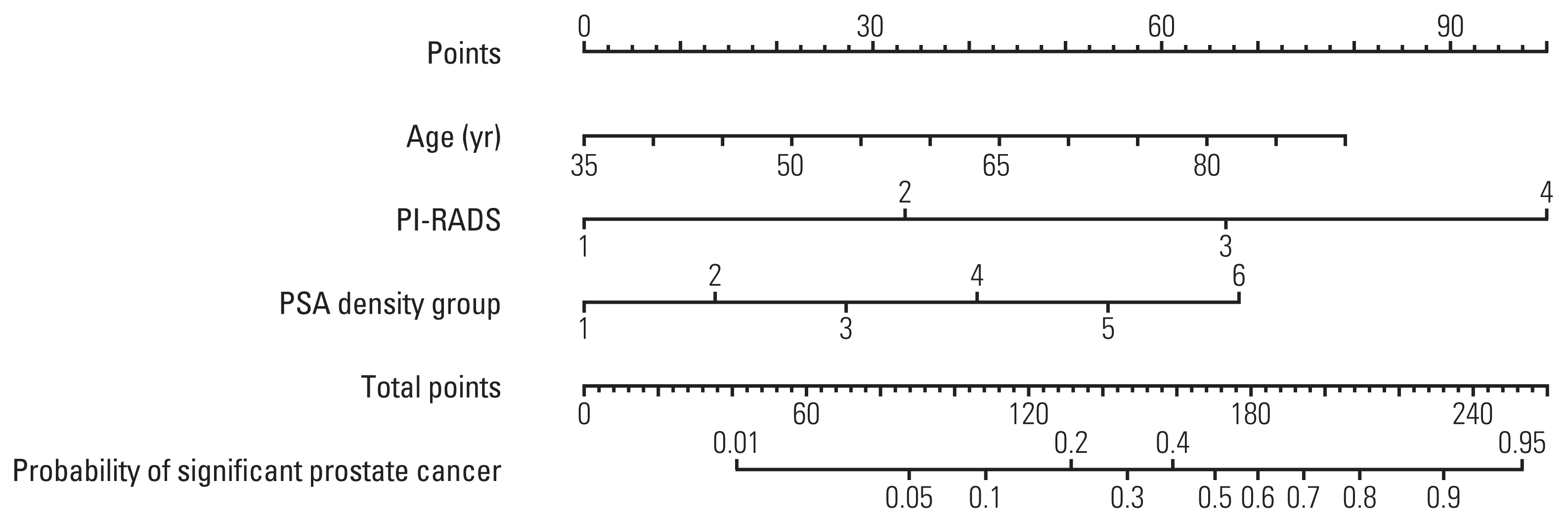
Nomogram of the predictive model for the probability of clinically significant prostate cancer (Gleason score ≥ 7 [3+4]). PI-RADS, Prostate Imaging Reporting and Data System; PSA, prostate-specific antigen.
For example, when a man is aged 65 years, has a PI-RADS score of 4 in bpMRI, and a PSAD of 0.17, the estimated probability of csPCa was calculated, using the equation, as 32.99% (Table 3).

Estimated probability of clinically significant prostate cancer
4. Internal and external validation of the nomogram for predicting csPCa
In internal validation, the nomogram showed good calibration with a slight overestimation of predicted probabilities after 0.4. The Hosmer-Lemeshow test produced a nonsignificant result (p=0.324), which supported the goodness-of-fit of the model. Likewise, in external validation, the nomogram showed good calibration with a slight underestimation of predicted probabilities between 0.3 and 0.7, and the Hosmer-Lemeshow test produced a nonsignificant result (p=0.303) (Fig. 2).

Internal and external validation. Hosmer-Lemeshow good-ness-of-fit test: Internal set: p=0.324, External set: p=0.303.
5. Decision curve analysis
On decision curve analysis, by combining bpMRI with clinical parameters (PSAD and age), the combination model showed a highest net benefit and net reduction in the number of false-positives among the strategies, for clinically relevant thresholds > 5%. “All” is the net benefit when all individuals are biopsied, and if the net benefit exceeds this value, it means that the pure true-positive value minus the number harmed is greater than when all are biopsied. A net benefit of 20% means that the marker is equivalent to a strategy that led to biopsy in 20 men per 100 men at risk, with all biopsy results testing positive for cancer. This combination model was equivalent to performing 25 biopsies per 100 men, without any negative biopsies (Fig. 3).

Net benefit decision curve. Net benefit=Benefit–(Harm× Exchange rate). The value excluding the false-positive rate from the true-positive rate of cancer, based on the high-risk threshold in the probability values estimated from the model. A net benefit of 20% means that the marker is equivalent to a strategy that led to biopsy in 20 men per 100 men at risk, with all biopsy results positive for cancer. “All” is the net benefit when all individuals are biopsied, and if it is greater than this value, pure true-positive minus harm is greater than the biopsy of all individuals. MRI, magnetic resonance imaging; PSAD, prostate-specific antigen density.
6. Unnecessary biopsies avoided and csPCa missed
Table 4 shows the number of unnecessary biopsies avoided, insignificant PCa diagnosed, and significant PCa missed, according to the threshold of probability. Applying a probability threshold of 7.5%, 21.6% of men could avoid prostate biopsy, while only 1.0% of csPCa cases would be missed.
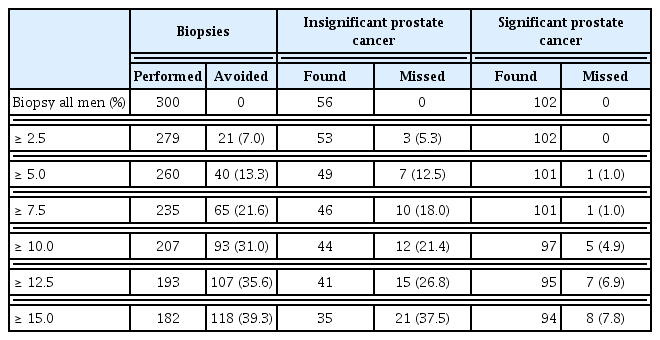
Unnecessary biopsies avoided and clinically significant prostate cancer missed
Discussion
To identify the potential risk of csPCa and reduce unnecessary prostate biopsies, current guidelines recommend the use of validated risk calculators (RCs) [21]. Risk stratification with multivariable RCs based on traditional clinical parameters (e.g., age, previous biopsy, family history, digital rectal examination) and PSA derivatives (e.g., free PSA, PSAD) as biomarkers have been proposed and adopted for making decisions in daily clinical practice [22,23]. These can stratify the risk of csPCa with relatively good reliability (AUC, 0.73 to 0.80), but might inform decisions for avoiding unnecessary prostate biopsies while sparing some patients from the diagnosis and morbidity of low-grade PCa [24]. However, the reliability is not sufficient for basing decisions in real clinical practice. To assist clinicians in making decisions about prostate biopsy, clinical tools, such as RCs, can be used to inform patients on an individual level, with high degrees of accuracy, generalizability, and validation.
To improve predictive abilities, RCs using novel biomarkers (e.g., selectMDX, Stockholm-3 [S3M]), blood-based markers (e.g., kallikrein), and urine-based markers (e.g., PCA3 and HOXC6) have been proposed [25]. Use of only these novel biomarkers did not yield high predictivity (AUC, 0.77 to 0.80). However, adding the novel biomarkers to clinical parameters resulted in an increase of the AUC to 0.87–0.89 [26]. Gains in net benefit must, however, be weighed against additional costs and the availability of tests, such as biomarkers and genomic markers [27].
Recently, mpMRI has taken on a role in the diagnosis and management of PCa, with a high sensitivity and negative-predictive value for csPCa. The findings of mpMRI impro-ved predictive accuracy by 9%, and it has been used as an important risk predictor in RCs. Several RCs based on mpMRI and clinical parameters have been proposed [10–12]. When magnetic resonance imaging (MRI) was incorporated into an RC, it showed superior diagnostic accuracy, reducing unnecessary biopsies while maintaining a level of sensitivity for csPCa comparable to that of other baseline predictive models [3]. A head-to-head comparison study was conducted between three representative RCs that incorporate mpMRI findings through extravalidation. The AUCs of the three novel models (MRI-ERSPC-3/4, ModRAD, and ModDis) were 0.82, 0.85, and 0.83 [28]. Moreover, it was reported that the ERSPC-RCs could reduce unnecessary biopsy by 36%, while missing high-grade PCa in 4% of men [12]. Thus, the implementation of an MRI-derived score into RCs currently appears to be the most promising approach for predicting the risk of csPCa.
The promising status of bpMRI for PCa diagnosis has recently been published [16–18]. In a previous study, we reported the diagnostic accuracy and value of bpMRI and transperineal bpMRI-US fusion prostate biopsy [19]. MpMRI consists of T2-weighted imaging, diffusion-weighted imaging, and dynamic contrast-enhanced (DCE) imaging. MpMRI is time-consuming (~40 minutes), expensive, and requires intravenous administration of contrast media. In contrast, bpMRI excludes DCE mode using contrast media from mpMRI, it could reduce the time for image acquisition and even the side effects that may occur due to the use of contrast media. Therefore, bpMRI is faster (~15 minutes), cheaper, and simpler than mpMRI, while retaining a sufficient diagnostic value [13]. In this multivariable RC, bpMRI also showed the highest predictability for csPCa among the single factors.
The strengths of RCs in this study was that it secured generalizability and applicability with reliable and discriminatory power (AUC, 0.861). We incorporated only bpMRI and clinical parameters routinely obtained prior to prostate biopsy. Risk assessments based on the combined predictive RC that included bpMRI and clinical parameters (age, PSAD) had comparable predictivity to the predictive model based on mpMRI (AUC, 0.797 to 0.850) and even a model with an added biomarker (AUC, 0.87 to 0.89) [10]. Additionally, clinical parameters such as age, prostate volume, PSA, and PSAD, are relatively easier to obtain in clinical practice, with no additional costs, whereas recently published laboratory assessments with genetic markers or biomarkers are expensive and laboratory-dependent. RCs that are based on less widely used risk predictors, such as genetic markers or biomarkers, will lead to decreased generalizability and applicability of the RCs in real clinical practice due to the cost and laboratory dependency.
This predictive RC showed high discriminatory power (AUC, 0.861) and yielded a great net benefit in decision curve analysis. When we applied a probability threshold of 7.5%, 21.6% of men could avoid prostate biopsy, while only 1.0% of csPCa cases were missed. At the probability threshold of 10.0%, it could reduce unnecessary biopsy by 31.0%, while missing csPCa in 4.9% of men. Furthermore, we achieved good calibration using bootstrap internal and external validation.
To the best of our knowledge, no previous RC has combined a bpMRI-derived score with easily obtained clinical parameters and used the results from advanced biopsy techniques (transperineal bpMRI-US fusion prostate biopsy). Our RCs were developed using data from a Korean population, where systematic PSA screening is not performed and where the cost of MRI is not covered by the health insurance system. Since PCa screening is widespread in the era of PSA, the role of MRI is emerging and the frequency of MRI use will increase. An individualized approach to PCa is needed, we believe that will be feasible through this RC.
The limitations of this study were its retrospective nature and accompanying bias. The study used data from a Korean population and was thus ethnically homogeneous; the effects of race therefore remain unclear. The other limitation lies in that this RC was developed from a single-arm study of bpMRI and clinical parameters, not a direct comparative study with the performance of RCs developed from mpMRI and clinical parameters, nor with biomarkers and genetic markers. Thus, head-to-head comparison trials are necessary to reach definite conclusion in the future.
A combined predictive model based on bpMRI and routinely obtained clinical parameters could predict csPCa with high discriminatory power (AUC, 0.861) and great net benefit. By implementing this RC, unnecessary prostate biopsies could be avoided while minimizing missed csPCa. This RC can provide measurable benefits and is useful with generalizability and applicability for clinical decision-making prior to prostate biopsies in real clinical practice.
Electronic Supplementary Material
Supplementary materials are available at Cancer Research and Treatment website (https://www.e-crt.org).
Notes
Ethical Statement
This study was approved by the ethics committee and the institutional review board of the KUMC (IRB No. 2018AN0339). Owing to its retrospective nature, the need to obtain informed consent was waived.
Author Contributions
Conceived and designed the analysis: Noh TI, Kang SH.
Collected the data: Noh TI, Hyun CW, Kang HE, Jin HJ, Tae JH, Shim JS, Sung DJ, Kang SH.
Contributed data or analysis tools: Noh TI, Kang SG, Cheon J, Lee JG, Kang SH.
Performed the analysis: Noh TI.
Wrote the paper: Noh TI.
Conflicts of Interest
Conflict of interest relevant to this article was not reported.
Acknowledgements
This research was supported by a grant from the Korea University College of Medicine, Seoul, Korea.