Prevalence and Prognostic Role of PIK3CA/AKT1 Mutations in Chinese Breast Cancer Patients
Article information
Abstract
Purpose
The prevalence of PIK3CA in Chinese breast cancer patients may be underestimated. Therefore, we investigated the distribution of somatic PIK3CA/AKT1 mutations in Chinese breast cancer patients and explored their roles in tumor phenotypes and disease prognosis.
Materials and Methods
Tumors from 507 breast cancer patients were prospectively collected from the West China Hospital between 2008 and 2013. Whole exons of AKT1 and PIK3CA were detected in fresh-frozen tumors using next-generation sequencing, and correlations between PIK3CA/AKT1 mutations and clinicopathological features were analyzed.
Results
The AKT1 mutation was found in 3.6% (18/507) of patients. Tumors from patients that carried the AKT1 mutation were estrogen receptor (ER)+/progesterone receptor (PR)+/human epidermal growth factor receptor 2 (HER2)‒ and were more likely to have high expression levels of Ki67. The prevalence of the PIK3CA mutation was 46.5% (236/507), and 35 patients carried two or three variants of the PIK3CA gene. PIK3CA mutations were associated with ER+/PR+/HER2‒ status. The prognosis of patients with one mutation in PIK3CA (or PIK3CA/AKT1) was not significantly different than that of patients with wild-type PIK3CA (or PIK3CA/AKT1), while patients with two or three variants in PIK3CA (or PIK3CA/AKT1) exhibited poorer outcomes in the entire group and in all three subgroups (ER+, HER2‒, Ki67 high), particularly with respect to overall survival.
Conclusion
A high frequency of somatic PIK3CA mutations was detected in Chinese breast cancer patients. In addition to the mutation frequency, the tumor mutational burden of the PIK3CA and AKT1 genes should also be of concern, as they may be associated with poor prognosis.
Introduction
The phosphoinositide 3-kinase (PI3K) signaling pathway, which promotes cancer cell growth and metabolism, is the most frequently mutated pathway in breast cancer. This pathway is associated with failure of clinical treatments, such as anti‒human epidermal growth factor receptor 2 (HER2) therapy and endocrine therapy, and chemotherapy resistance [1,2]. Clinical development of several pan-PI3K inhibitors, PI3Kα subunit-specific inhibitors, PI3Kβ subunitspecific inhibitors, mammalian target of rapamycin (mTOR) inhibitors, and PI3K/mTOR dual inhibitors is currently underway. However, the biomarkers to evaluate the efficacy of these agents still need to be elucidated.
According to The Cancer Genome Atlas network (TCGA), the percentage of PIK3CA mutations is 34.18%, and the percentage of AKT1 mutations is 3.14% [3]. Reports of the prevalence of PIK3CA mutation varied among studies (15.6%-47.6%) [4-16], and the percentage PIK3CA mutation is between 15.6% and 28.3% in Chinese breast cancer patients [10,11,14]. These mutation frequencies may be underestimated. One possible reason is that most studies detected several exons with hotspot mutations via Sanger sequencing, spectrometry genotyping, or hydrolysis probe assays [4-13]. In the BOLERO-2 trial, tumor samples from 302 patients were analyzed via next-generation sequencing (NGS). In this trial, the percentage of PIK3CA mutations was 47.6%, which is within the range of the most frequently mutated genes in breast cancer [15]. Another possible reason is that some studies used formalin-fixed, paraffin-embedded (FFPE) tissues [7,10,13], and as preservation time increases, DNA may break down and therefore may not be amplified. In a previous study, we also detected PIK3CA and AKT1 hotspot mutations using FFPE tissues from 288 breast cancer patients via Sanger sequencing. However, the amplification failure rate of a single exon was as high as 25.7%, where the frequency of PIK3CA mutation was only 15.6% [10]. Both aforementioned reasons can lead to underestimation of the PIK3CA mutation frequency.
In this single-center observational study, we investigated the frequency of PIK3CA and AKT1 mutations in tumor tissues from 507 Chinese breast cancer patients using NGS and explored their role in tumor phenotype and disease prognosis.
Materials and Methods
1. Study patients
All patients pathologically diagnosed with breast cancer were prospectively registered in the Breast Cancer Information Management System (BCIMS) at the West China Hospital, Sichuan University beginning in 2008. In this study, patients who had undergone surgery between 2008 and 2013 were recruited. Patients who underwent neoadjuvant chemotherapy, lacked complete clinical information, or were unable to provide enough frozen tumor tissue were excluded from this study. Ultimately, 507 patients were eligible for the PIK3CA/AKT1 mutation test and analysis of clinical characteristics.
Clinical and pathological characteristics of 507 patients were extracted from the BCIMS (S1 Table). Immunohistochemistry (IHC) scoring for estrogen receptor (ER), progesterone receptor (PR) was conducted following the Guidelines for Testing of ER and PR in Breast Cancer [17]; IHC and fluorescence in situ hybridization scoring for human epidermal growth factor receptor-2 (HER2) was performed according to the Guidelines for HER2 Detection in Breast Cancer [18]. The subtypes of breast cancer were classified according to St. Gallen International Expert Consensus [19]. Follow-up on survival status was available until May 2017. Invasive disease-free survival (iDFS) was defined as the interval between surgery date and first relapse of cancer, death, the second primary tumor, or last follow-up [20]. Overall survival (OS) was defined as the interval between surgery date and patient death, or last follow-up. Among 498 patients with stage I-III breast cancer, 57 iDFS events and 36 OS events were observed.
2. Targeted DNA sequencing and bioinformatics
Freshly frozen tumor tissues were obtained from the 507 breast cancer patients. Tumor content of ≥ 50% was qualified via pathology quality control. Tumor DNA samples were screened for variants in all coding exons of the PIK3CA and AKT1 genes with a customized QIAGEN Gene Read panel, using NGS on a MiSeq system (Illumina, San Diego, CA). Whole blood or distal adjacent normal tissue were used to filter out germline variants for 24 patients in which novel PIK3CA variants were identified during interim data analysis.
After trimming adapters and low-quality bases (sequencing quality cutoff at Q30), reads were mapped to Human B37.3. Genomic variants were organized using the following criteria: reads uniquely mapped to the genome; mapping quality > 15; number of mutated reads ≥ 5, and mutant allele frequency ≥ 0.01. Variants were then manually verified in the Genome Browser.
3. Statistical analysis
Two-tailed t test, chi-square test, and Fisher exact test were performed to assess significance of the association between variables (PIK3CA and AKT mutations) and clinical characteristics (SPSS ver. 20, IBM Corp., Armonk, NY). The Kaplan-Meier survival curve was drawn and tested by log-rank test to evaluate the differences in iDFS and OS between the variables. The effect of mutations on prognosis was analyzed by Cox multivariate risk models. A p-value of < 0.05 was considered statistically significant.
4. Ethical statement
This study was approved by the Clinical Test and Biomedical Ethics Committee of West China Hospital, Sichuan University. Written informed consent was provided by all patients.
Results
1. Prevalence and characteristics of PIK3CA and AKT mutations
The prevalence of PIK3CA and AKT1 mutations is shown in Table 1. AKT1 mutation was found in 18 patients (3.6%), and the percentage of hotspot mutations for AKT1_E17K was 3.4% (17/507). PIK3CAmutation was detected in 236 (46.5%) patients. PIK3CA hotspot mutations (H1047R/L, E545K, E542K) were found in 39.4% of breast cancer patients (200/507), with H1047R ranking the highest. These hotspot mutations account for 84.7% of breast cancer patients (200/236) who carry somatic PIK3CA variants. There were 273 mutations of PIK3CA in total. Thirty-five patients carried two or three mutations in PIK3CA (S2 Table), and 33 had concurrent hotspot mutations with 1 or 2 non-hotspot mutations. AKT1 mutations (3 AKT1_E17K and 1 AKT1_C77F) were concurrent with PIK3CA_H1047Rmutation in four patients. When AKT1 and PIK3CAmutations were combined based on mutant burden, 39 patients carried two or three mutations (2MTs) (S2 Table), 211 patients had one mutation (1MT), and 257 patients carried wild-type (WT) PIK3CA and AKT1. The clinical and pathological features of patients with PIK3CA and AKT1 mutations are shown in Table 2.
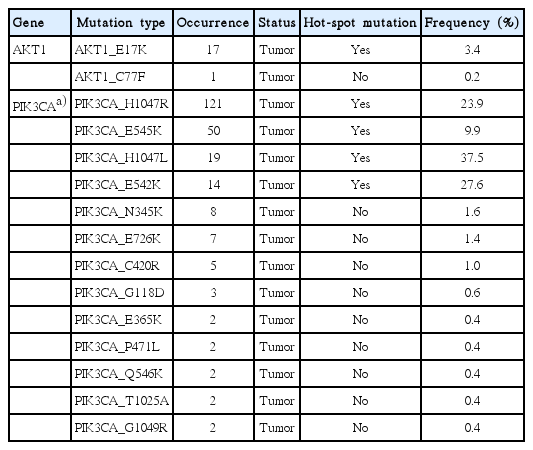
PIK3CA and AKT1 mutations in 507 breast cancer patients
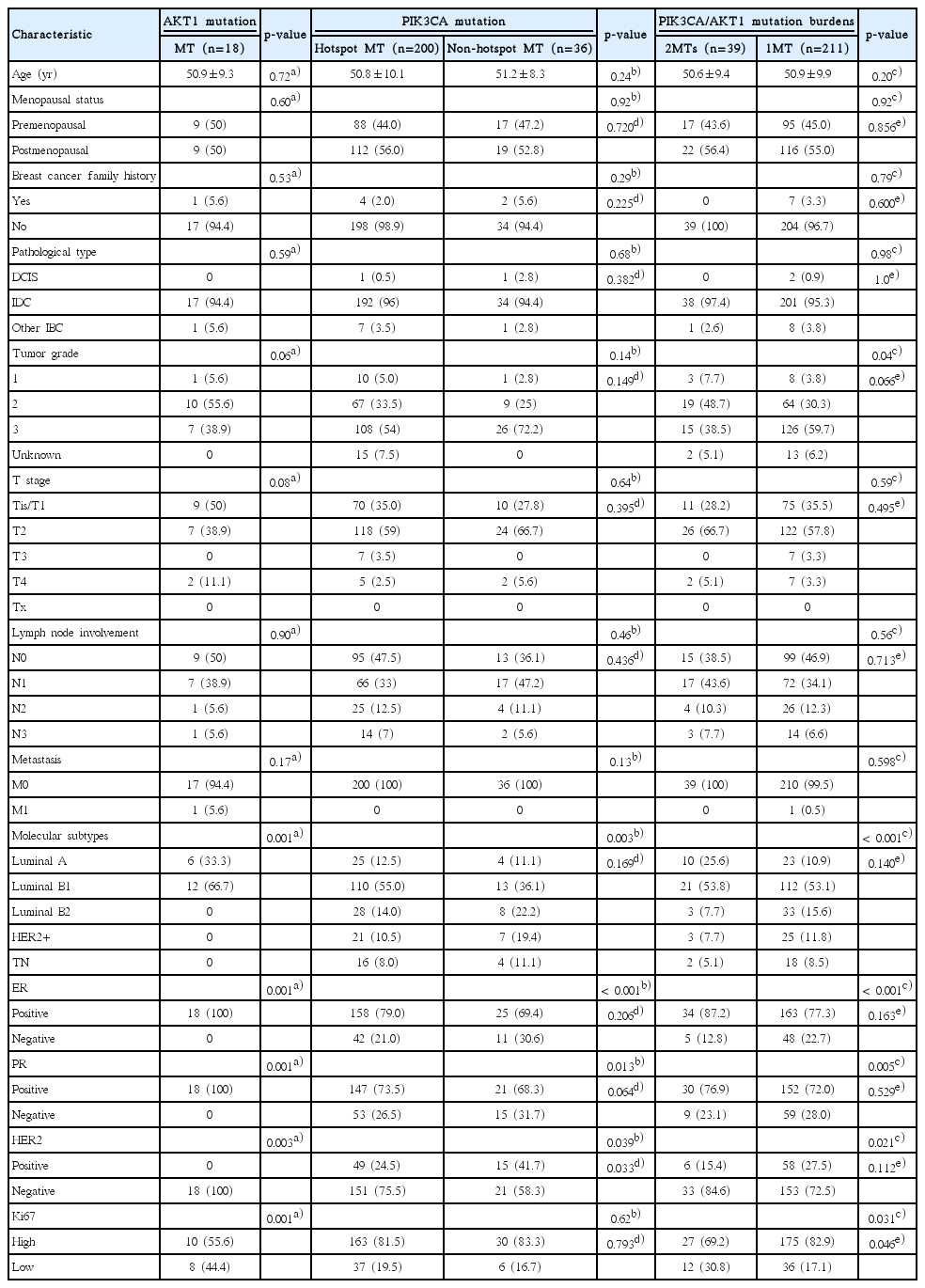
The clinical and pathological features of patients with PIK3CA and AKT1 mutations
1) AKT1 mutation
All patients with AKT1mutations were ER+/PR+/HER2– (Table 2). In addition, the AKT1 E17K mutation was significantly associated with Ki67 high expression, but was not associated with age at diagnosis, menopausal status, family history, pathological type, tumor grade, T category, lymph node stage or metastasis.
2) PIK3CA mutation
Compared to breast cancers expressing wild type PIK3CA, both hotspot and non-hotspot PIK3CA mutant cancers were more likely to be ER+, PR+, HER2– or of the luminal B (HER2 negative) subtype (Table 2). PIK3CA mutation was not associated with age at diagnosis, menopausal status, family history, pathological type, tumor grade, T category, lymph node stage, Ki67 expression, or metastasis. No difference was observed between patients with hotspot mutations and nonhotspot mutations, except for HER2 status.
3) PIK3CA/AKT1 mutation
When AKT1 and PIK3CA mutations were analyzed by mutation burden, cancers with 2MTs or with 1MT were more likely to be ER+, PR+, HER2–, high Ki67, or of the luminal B (HER2 negative) subtype compared with cancers with WT PIK3CA and AKT1. When 2MTs and 1MT were sub-analyzed, no difference was observed between the two subgroups except for Ki67 expression.
2. Association of PIK3CA and AKT1 mutations with survival
Survival analysis was conducted among 296 invasive stage I-III breast cancer patients with at least a 5-year follow-up. According to the tumor mutational burden of PIK3CA/AKT1, there were 18 patients with 2MTs, 124 cases with 1MT and 154 cases with WT. The baseline of these 296 patients is summarized in S3 Table. Both PIK3CA and PIK3CA/AKT1 mutations were more frequent in cancers that were ER+, HER2–, or expressing high Ki67. The Kaplan-Meier survival curve and Cox multivariate risk models were used to evaluate the survival of patients.
1) Total patients (296 cases)
Regarding PIK3CAmutation, patients with 1MT showed better iDFS than patients with 2MTs (Fig. 1A), with a relative hazard ratio (HR) of 0.344 (p=0.049) after adjustment (Table 3). Patients with 1MT (adjusted HR, 0.222; p=0.020) or WT PIK3CA (adjusted HR, 0.221; p=0.021) had better OS than patients with 2MTs (Table 3, Fig. 1B). However, there was no difference in iDFS between patients with WT and 2MTs (Fig. 1A). In addition, no difference in iDFS or OS was observed between patients with WT and 1MT of PIK3CA (Fig. 1A and B).

Impact of PIK3CA/AKT1 mutations on the invasive disease-free survival (iDFS) and overall survival (OS) of 296 breast cancer patients with stage I-III and at least 5-year follow-up. Kaplan-Meier survival analysis; p-values calculated using a log-rank analysis. Estimated iDFS and OS by mutant burden: iDFS (A) and OS (B) for patients with wild-type (WT), one mutation (1MT), and two or three mutations (2MTs) of PIK3CA; iDFS (C) and OS (D) for patients with WT, 1MT, and 2MTs of PIK3CA/AKT1.
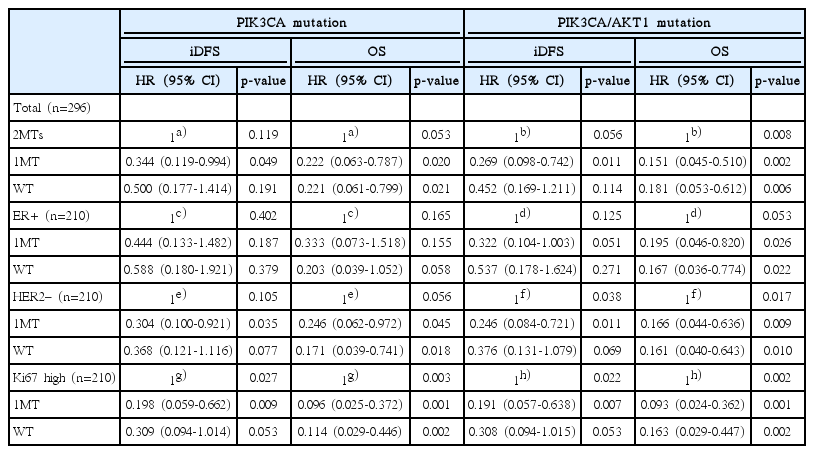
Cox multivariate risk model for patients with different mutant burdens (stage I-III and at least 5-year follow-up)
Regarding PIK3CA/AKT1 mutation, patients with 1MT exhibited better iDFS (adjusted HR, 0.269; p=0.011) and OS (adjusted HR, 0.151; p=0.002) than those with 2MTs (Table 3, Fig. 1C and D). Patients with WT PIK3CA/AKT1 exhibited a better OS than those with 2MTs (adjusted HR, 0.181; p=0.006) (Table 3, Fig. 1D), but no significant difference in iDFS. While patients with 1MT in PIK3CA/AKT1 showed a trend toward better iDFS than patients with WT PIK3CA/AKT1 (p=0.054) (Fig. 1C), the OS of patients with 1MT in PIK3CA/AKT1 was not significantly different than in patients with WT PIK3CA/AKT1 (Fig. 1D).
2) ER-positive patients (210 cases)
Regarding the PIK3CA gene, no significant difference in iDFS was observed among ER+ patients with WT, 1MT, and 2MTs in PIK3CA (Fig. 2A). Patients with WT PIK3CA had a trend of better OS than those with 2MTs in PIK3CA (adjusted HR, 0.203; p=0.058) (Table 3, Fig. 2B). However, there was no difference in OS for patients with WT and 1MT in PIK3CA (Fig. 2B).

Impact of PIK3CA/AKT1 mutations on the invasive disease-free survival (iDFS) and overall survival (OS) of 210 estrogen receptor (ER) positive breast cancer patients with stage I-III and at least 5-year follow-up. Kaplan-Meier survival analysis; p-values calculated using a log-rank analysis. Estimated iDFS and OS by mutant burden: iDFS (A) and OS (B) for patients with wild-type (WT), one mutation (1MT), and two or three mutations (2MTs) of PIK3CA; iDFS (C) and OS (D) for patients with WT, 1MT, and 2MTs of PIK3CA/AKT1.
Regarding PIK3CA/AKT1 mutation, ER+ patients with 1MT showed marginally better iDFS (adjusted HR, 0.322; p=0.051) and significantly better OS (adjusted HR, 0.195; p=0.026) than those with 2MTs (Table 3, Fig. 2C and D). Patients with WT PIK3CA/AKT1 exhibited better OS than those with 2MTs in PIK3CA/AKT1 (adjusted HR, 0.167; p=0.022) (Table 3, Fig. 2D), but no significant difference in iDFS (Fig. 2C). The iDFS and OS of patients with 1MT were not significantly different from those with WT PIK3CA/AKT1 (Fig. 2C and D).
3) HER2-negative patients (210 cases)
Regarding PIK3CA mutation, HER2– patients with 1MT exhibited significantly better iDFS (adjusted HR, 0.304; p=0.035) and OS (adjusted HR, 0.246; p=0.045) than those with 2MTs (Table 3, Fig. 3A and B). Patients with WT PIK3CA had better OS (adjusted HR, 0.171; p=0.018) and showed a trend toward better iDFS (adjusted HR, 0.368; p=0.077) than those with 2MTs in PIK3CA (Table 3, Fig. 3A and B). No difference in iDFS or OS was observed between patients with WT and 1MT in PIK3CA (Fig. 3A and B).
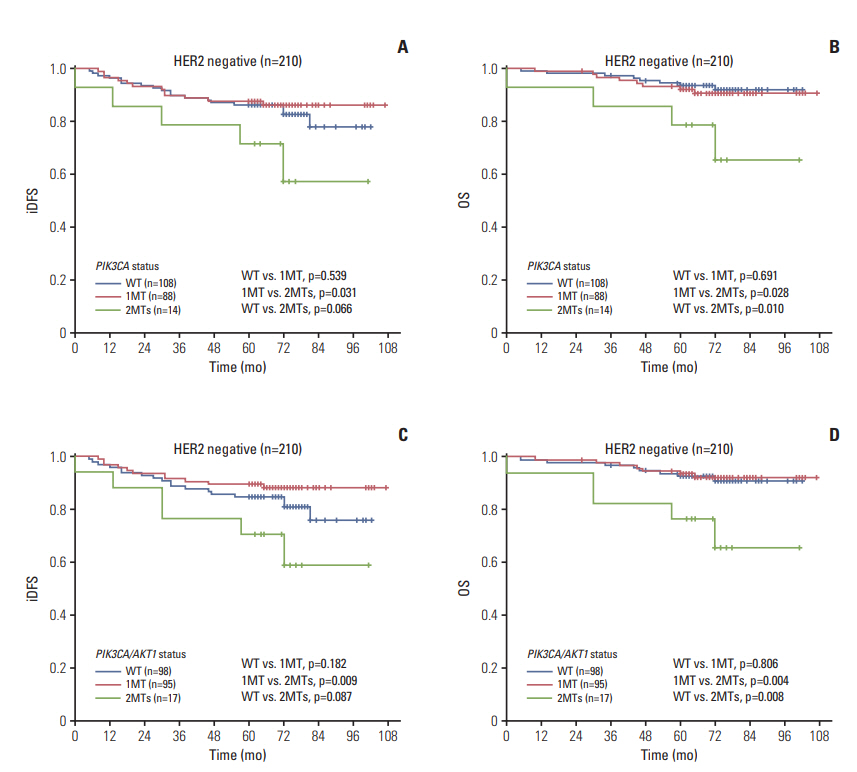
Impact of PIK3CA/AKT1 mutations on the invasive disease-free survival (iDFS) and overall survival (OS) of 210 human epidermal growth factor receptor 2 (HER2) negative breast cancer patients with stage I-III and at least 5-year followup. Kaplan-Meier survival analysis; p-values calculated using a log-rank analysis. Estimated iDFS and OS by mutant burden: iDFS (A) and OS (B) for patients with wild-type (WT), one mutation (1MT), and two or three mutations (2MTs) of PIK3CA; iDFS (C) and OS (D) for patients with WT, 1MT, and 2MTs of PIK3CA/AKT1.
Regarding PIK3CA/AKT1 mutation, HER2– patients with 1MT had better iDFS (adjusted HR, 0.246; p=0.011) and OS (adjusted HR, 0.166; p=0.009) than those with 2MTs (Table 3, Fig. 3C and D). Patients with WT PIK3CA/AKT1 had better OS (adjusted HR, 0.161; p=0.010) and showed a trend toward better iDFS (adjusted HR, 0.376; p=0.069) than those with 2MTs (Table 3, Fig. 3C and D). There was no difference in iDFS and OS between patients with WT and 1MT in PIK3CA/AKT1.
4) Patients with high expression of Ki67 (240 cases)
Regarding PIK3CA mutation, patients with high expression of Ki67 and 1MT had better iDFS (adjusted HR, 0.198; p=0.009) and OS (adjusted HR, 0.096; p=0.001) than those with 2MTs (Table 3, Fig. 4A and B). Patients with WT PIK3CA exhibited better OS than those with 2MTs in PIK3CA (adjusted HR, 0.114; p=0.002) (Table 3, Fig. 4B), with no significant difference in iDFS. The iDFS and OS of patients with 1MT were not significantly different than in patients with WT PIK3CA (Fig. 4A and B).
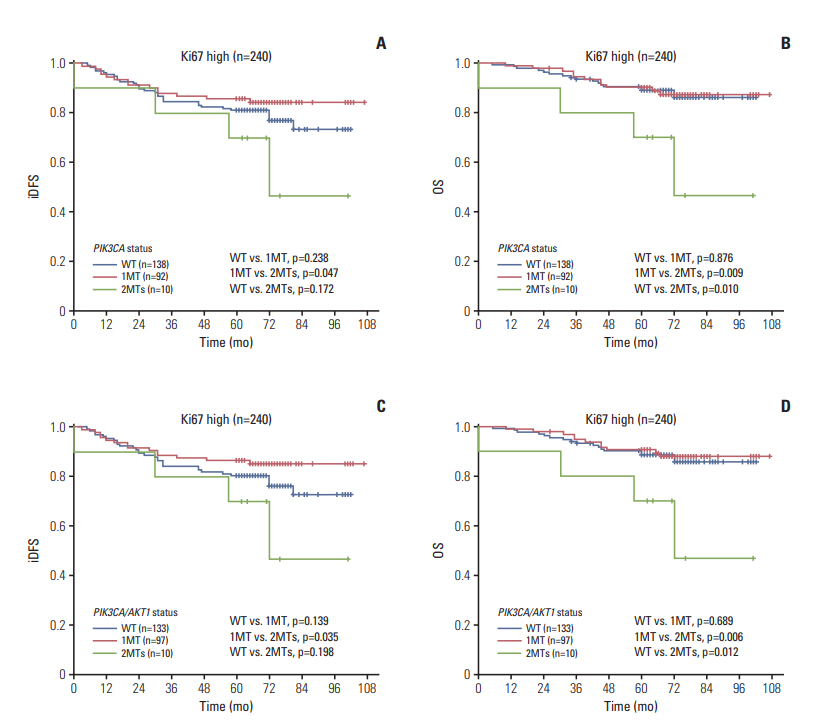
Impact of PIK3CA/AKT1 mutations on the invasive disease-free survival (iDFS) and overall survival (OS) of 240 Ki67 high breast cancer patients with stage I-III and at least 5-year follow-up. Kaplan-Meier survival analysis; p-values calculated using a log-rank analysis. Estimated iDFS and OS by mutant burden: iDFS (A) and OS (B) for patients with wild-type (WT), one mutation (1MT), and two or three mutations (2MTs) of PIK3CA; iDFS (C) and OS (D) for patients with WT, 1MT, and 2MTs of PIK3CA/AKT1.
Regarding PIK3CA/AKT1mutation, patients with 1MT had better iDFS (adjusted HR, 0.191; p=0.007) and OS (adjusted HR, 0.093; p=0.001) than those with 2MTs (Table 3, Fig. 4C and D). Patients with WT PIK3CA/AKT1 exhibited better OS (adjusted HR, 0.163; p=0.002) and a trend toward better iDFS (adjusted HR, 0.308; p=0.053) than those with 2MTs (Table 3, Fig. 4C and D). No difference in iDFS or OS was observed between patients with 1MT and WT PIK3CA/AKT1.
The prognosis between patients with mutant (hotspot and non-hotspot) and WT PIK3CA genes was also compared. Results showed that the iDFS and OS of patients with mutant PIK3CA was not significantly different from patients with WT PIK3CA, whether they were in the entire group or one of the three subgroups (ER+, HER2–, Ki67 high) (S4-S7 Figs.). Survival was also evaluated among patients with hotspot MT, non-hotspot MT and WT PIK3CA, and there was no difference in iDFS or OS (S4-S7 Figs.).
Survival between patients with mutant and WT AKT1 was also evaluated, and there was no difference in iDFS or OS, whether they were in the entire group or one of the 3 subgroups (S8 Fig.). In addition, we compared iDFS and OS between patients with mutant (2MTs plus 1MT) or WT PIK3CA/AKT1, and no significant difference was observed (S9 Fig.).
Discussion
This study provided new insight into the complexity of PIK3CA and AKT1 mutations in Chinese breast cancer patients. AKT1 mutations were detected in 3.6% of the 507 patients, and 4.9% (18/370) in the luminal subtype, which is similar to the 3.14% in the TCGA report [3]. PIK3CA mutations were detected in 46.5% of the 507 patients, and the hotspot mutations of PIK3CA were 39.4%. The frequency of PIK3CA mutations was 50.8% (188/370) in the luminal subtype, 41.8% (28/67) in the HER2-positive subtype, and 28.6% (20/70) in triple-negative breast cancer. This was similar to the PIK3CA mutation rates of BOLERO-2 trial, which was also detected via NGS [15]. In contrast, this was significantly higher than the PIK3CA mutation rates previously reported in a cohort of 729 Chinese women with breast cancer (28.3%) [11], as well as what was reported in a cohort of HER2-amplified metastatic breast cancer (24%) [14], which only detected hotspot mutations of PIK3CA. These results illustrated that NGS is a reliable method that can detect PIK3CA and AKT1 mutations efficiently.
Also, we confirmed significant associations of AKT1 mutations with clinicopathological and molecular characteristics, as well as PIK3CAmutations (whether hotspot or nonhotspot mutations). Both AKT1 mutations and PIK3CA mutations were significantly associated with ER positive, PR positive and HER2 negative. AKT1 mutations were also associated with high Ki67 expression. But Ki67 expression was not different among patients harboring hotspot mutation, non-hotspot mutation, or WT PIK3CA. This is consistent with the literature [6,7,12,21].
The association between PIK3CAmutations and prognosis has been evaluated by many studies. However, results from these studies are still inconclusive. Some studies showed favorable [6,7,22], and others showed adverse [4,6,10,14,23-25], impacts of PIK3CA mutations on patient outcomes, while a significant number of reports did not show any prognostic significance [5,8,9,11-13,26]. In HER2-positive breast cancers, PIK3CA mutation was associated to poor prognosis in several studies [4,25,27], while the association of PIK3CA mutation with prognosis was not significantly in the FinHER trial [5]. PIK3CAmutation predicted poorer pathologic complete response (pCR) in patients with HER2+ breast cancer treated with neoadjuvant therapies [8,9,11,28]; however, the association of PIK3CA mutation with pCR did not translate into DFS or OS outcomes [29,30]. In the present study, patients with 1MT of the PIK3CA gene did not have significantly different iDFS or OS when compared to those with WT PIK3CA, whether they were in the entire group or all three subgroups (ER+, HER2–, Ki67 high). In addition, PIK3CA mutation was not associated with prognosis of HER2-positive patients (WT vs. MT, PDFS=0.268, POS=0.842, data not shown). These results demonstrated that single PIK3CA gene mutation might have little effect on the prognosis of breast cancer patients.
Preclinical models found PIK3CA mutations alone, compared to PTEN loss or AKT1 mutations, can cause weaker or more inconsistent activation of PI3K-AKT signaling [31,32]. If this signaling pathway accumulates more genetic alteration burden, it may lead to higher activation of the pathway. For prognosis, patients simultaneously harboring both PIK3CAmutation and PTEN loss had lower DFS and OS [12], which suggest that it may be possible to analyze the prognosis of patients according to the genetic alteration burden of PI3K-AKT pathway. In the present study, we compared prognosis of patients with 2MT of PIK3CA/AKT1 to those with 1MT or wild-type PIK3CA/AKT1, which showed 2MT of PIK3CA/AKT1 caused poorer iDFS and OS. Patients with 2MT of PIK3CA also had poorer prognosis. These results suggested that greater number of alterations in PI3K/AKT/mTOR pathway might cause higher activation of this pathway, which was associated with poor prognosis.
Drugs targeting the PI3K/AKT/mTOR pathway in breast cancer are widely known, and some of them are approved for use in ER+ advanced breast cancer. Several studies have attempted to determine in which patients these drugs would achieve better clinical efficacy. An exploratory analysis using tumor samples from the BOLERO-2 trial showed that the efficacy of everolimus was largely independent of the most commonly altered genes (PIK3CA, FGFR1 and CCND1) in hormone receptor-positive and HER2-negative breast cancer. Subgroup analysis showed that PIK3CA exon-9 mutations were associated with a greater benefit from everolimus than exon-20 mutations [15]. However, another study using cellfree DNA from plasma samples from the BOLERO-2 trial showed that everolimus prolonged median progression-free survival in patients with PIK3CA H1047R and E545K/E542K mutations to a similar degree [33]. These different results demonstrate that more accurate and effective biomarkers are still needed to determine the efficacy of drugs targeting the PI3K/AKT/mTOR pathway.
There are some limitations to the present study. This was a single-center retrospective study with a relatively small sample size. Although the present study found that a tumor mutational burden of 2-3 in PIK3CA/AKT1 was associated with poorer outcomes, the sample size in this subgroup was relatively small compared to patients with WT or 1MT in PIK3CA/AKT1. The active burden for the entire PI3K/AKT1/mTOR pathway should be evaluated in a larger sample with a longer follow-up time.
In summary, PIK3CA/AKT1 mutation was detected using NGS in 49.3% of breast cancer patients from a single hospital in West China, with the highest mutation frequency in the luminal cancers. PIK3CA/AKT1 mutation was associated with positive ER, positive PR, or negative HER2 expression status. The prognosis of patients with one mutation in PIK3CA (or PIK3CA/AKT1) was not significantly different than in WT patients. Patients with a tumor mutational burden of 2-3 in PIK3CA (or PIK3CA/AKT1) had poorer prognosis in the entire group, or all 3 subgroups (ER+, HER2–, Ki67 high), particularly with respect to OS. These findings suggest that, in addition to mutation frequency, the tumor mutational burden of the PIK3CA and AKT1 genes should also be considered, and that these could be potential prognostic biomarkers in breast cancer patients.
Electronic Supplementary Material
Supplementary materials are available at Cancer Research and Treatment website (https://www.e-crt.org).
Notes
The authors have read the journal's policy and have the following competing interests: Xuehua Zhu, Yun Sun, Jiemin Wang and Min Hu were employees of Dizal Pharmaceutical during this study. The remaining authors declare that they have no competing interests. This does not alter the authors' adherence to Cancer Research and Treatment policies on sharing data and materials.
This work was supported by Dizal Pharmaceutical (Recipient: Z.H.). The funder provided support in the form of salaries for authors (X.H.Z., Y.S., J.M.W., and M.H.), but did not have any additional role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgements
We would like to thank LetPub (www.letpub.com) for providing linguistic assistance during the preparation of this manuscript.