Epidemiology of Intracranial Metastases in Korea: A National Cohort Investigation
Article information
Abstract
Purpose
To investigate the epidemiologic features of intracranial metastases (ICMET) in Korea, we performed a cohort study using the National Health Insurance Service–National Sample Cohort database, which comprised healthcare usage information of approximately 1 million Korean individuals over 12 years.
Materials and Methods
We enrolled 998,602 subjects, after excluding 18,218 subjects diagnosed with any cancer during the washout period (2002-2004). The observation period was 9 years (2005-2013; 8,725,438 person-years). The initial diagnosis date of ICMET and the primary cancer was recorded. The incidence was determined based on the number of incident cases and observation size, whereas survival was estimated using death statistics from the database.
Results
Through observation period, a total 776 subjects developed ICMET. The age-standardized incidence of ICMET was 8.2 per 100,000 person-years. The mean interval between the initial diagnosis date of the primary cancer and ICMET was 13.1 months. Patients with ICMET had shorter survival than those without ICMET (30.9 months vs. 81.4 months, p < 0.001). The ICMET incidence among the cancer patients was 5.0 per 1,000 person-years; it was highest in lung cancer cases, followed by breast and liver cancer cases. Moreover, ICMET from lung cancer was the most common metastasis type, followed by ICMET from liver and breast cancer.
Conclusion
The incidence of ICMET was 8.2 per 100,000 person-years among the Korean population and 5.0 per 1,000 person-years among cancer patients. Most of the ICMET cases arose from lung cancer. ICMET also critically influenced survival in cancer patients.
Introduction
Cancer is a life-threatening disease, and metastasis is the major cause of morbidity and mortality among cancer patients. Among the various neurologic complications of cancer, intracranial metastasis (ICMET) is the most common and devastating one. Although ICMET can spread to all intracranial structures, including the cranium and meninges, the most common site is the brain parenchyma [1]. With the increase in the life expectancy of the population and improvements in cancer treatment, the burden of ICMET treatment has also increased [2].
However, the epidemiology of ICMET has only been reported in a few population-based reports in the United States and Europe [2-7]; its reported incidence ranges from 7.0 to 15.7 per 100,000 person-years according to the study methodology used. To our knowledge, no epidemiologic reports regarding ICMET in Korea have been published, despite the presence of a well-established Korea Central Cancer Registry since 1980. Although the cancer statistics in Korea have been reported annually from this registry [8,9], these reports mainly focus on the primary cancer statistics.
In order to assess the epidemiologic features of ICMET in Korean individuals, we conducted a retrospective cohort study using the National Health Insurance Service–National Sample Cohort (NHIS-NSC) database, which comprised healthcare usage information of approximately 1 million individuals of the Korean population over a 12-year period [10].
Materials and Methods
1. NHIS-NSC
The NHIS-NSC was established through the random selection of 2% of all individuals enrolled in the NHIS—the single universal insurer in Korea. In the random selection procedure, subjects were stratified by sex, age, and socio-economic status. Approximately 97% of the entire population is covered by the NHIS. Hence, this sample cohort can be considered to represent the national Korean population. The Korean population registry identification number was substituted with a newly assigned identification number to mask personal information. From 2002 to 2013, all healthcare usage information, including any diagnosis based on the Korean Standard Classification of Diseases (KCD) code, the date of healthcare usage, and the related expense of each item, was recorded. Information regarding the demographic factors and death was also extracted.
2. Cohort design for the assessment of ICMET
The maintenance of a sufficient washout period is essential to accurately estimate the incidence of a disease in a cohort study. Accordingly, we set the enrollment date as January 1, 2005, in order to obtain a washout period of 3 years (2002-2004). A total of 1,016,820 subjects were initially enrolled. Among these subjects, 18,218 who were diagnosed with any cancer (Cxx as per the KCD code) from 2002 to 2004 were excluded. Thus, a total of 998,602 subjects were initially registered. The total observation period was 9 years (2005-2013). Although the original NHIS-NSC was designed as a dynamic cohort, the dead subjects in the present study were not replaced by newborn children, in order to maintain a fixed initial enrollment.
This study was approved by the database provider (NHIS-2016-2-260). The need for study approval was waived by the institutional review board (X-1611-372-906), as the study used an anonymized public database that is available to researchers.
3. Definition of terms used
The primary endpoint was set as the first date of the diagnosis of ICMET (C793 or C7930, metastasis to the brain; C7931, metastasis to the meninges). To determine the primary cancer related to the ICMET, the first date of the diagnosis of any cancer (Cxx), excluding ICMET, was also extracted. In cases where subjects had multiple primary diagnostic codes, the earliest diagnosis was registered and categorized.
Primary cancers were classified as 24 entities according to the Korea Central Cancer Registry (Table 1) [8]. The date of diagnosis associated with the primary cancer was also recorded. Ages from 0 to 79 years were classified at 10-year intervals, and those aged > 80 years were assigned to a single separate group at registration. The date of death was recorded for the dead subjects.
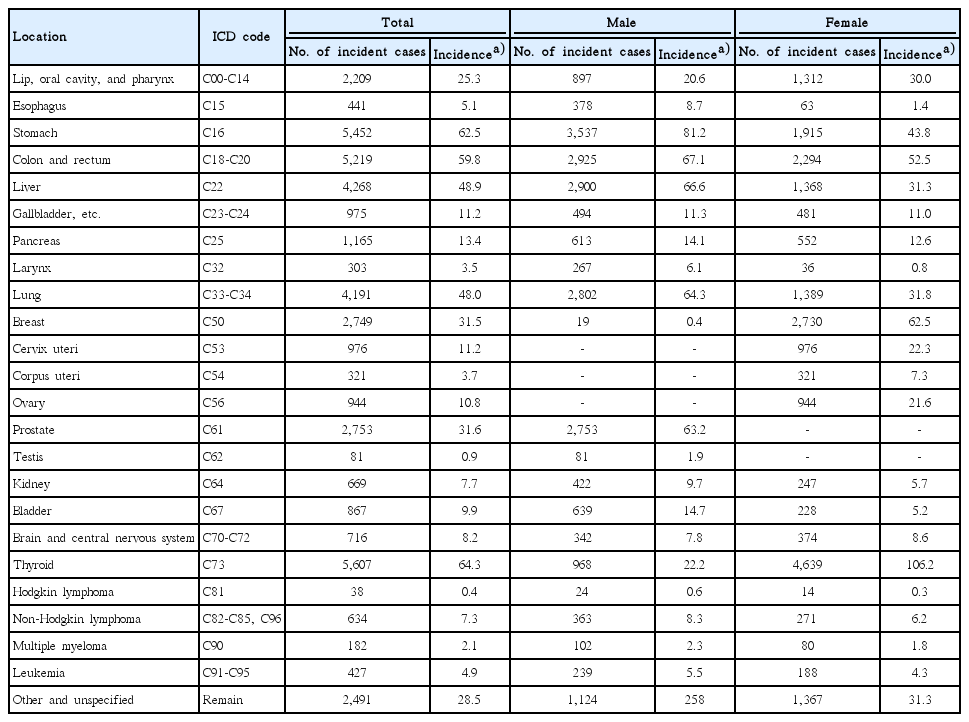
Cancer incidence by primary location
4. Statistical analysis
We used open source structured query language, MariaDB (ver. 10.1.17, MariaDB foundation, http://mariadb.org), for data manipulation and extraction. Moreover, R software ver. 3.3.1 (the Foundation for Statistical Computing, http://www.r-project.org), with suitable packages (survival, http://cran.r-project.org/package=survival), was used for statistical analysis.
The incidence was calculated as [Number of diagnosed subjects/Total observation period (person-years)]×(100,000 or 1,000). And, the confidence interval (CI) of the crude incidence was calculated using the Mid-P exact test [11]. Standardization according to age-group was conducted using the new World Health Organization world standard population 2000-2025 guidelines (Fig. 1) [12]. The survival duration was analyzed using Kaplan-Meier survival analysis. Cancer survival and ICMET survival were determined as the interval from the date of the initial diagnosis of the primary cancer and ICMET to the date of death or last observation date of the cohort (December 31, 2013), respectively.
Heatmap of the population structures. The proportion of each age group is presented as a percentage. The population structure of this cohort is very similar to that generated by the Korean census 2005 data. However, the World Health Organization (WHO) 2000-2025 population structure is markedly different from both these population structures.
The cancer-specific incidence of ICMET was analyzed only for cancers with > 2,600 incident cases. When the number of all incident cancer patients (n=43,678) and all ICMET patients (n=776) were considered, ICMET patients were found to represent only 1.8% of all cancer patients. Based on the proportion of 1.8±0.5% with suitable 95% confidence levels, the required sample size was estimated as > 2,558 [13]. Hence, stomach, colorectal, liver, lung, breast, prostate, and thyroid cancer cases were also included in the sub-group analysis. Comparison of survival was performed for cancers with ≥ 30 ICMET patients.
The survival duration was generally expressed as mean survival±standard error. In the present study, the median survival duration could not be estimated, as > 50% patients with any cancer (thyroid, breast, ovary cancer, and others) survived for the entire observation period. Hence, we unified the expression of the survival function as mean survival. However, the 5-year survival rate was also provided as supplementary information. To estimate survival among those diagnosed with ICMET, the median value of survival was used. The comparison of the survival function was performed using the log-rank test. In general, a p-value of < 0.05 was considered as statistically significant.
Results
1. Overall results
Of 998,602 subjects enrolled, 41,032 died during the observation period. Thus, the total observation size of this cohort was 8,725,438 person-years. The proportions of the population according to age and sex were similar, based on comparisons with the population and housing census in 2005 (Fig. 1). A total of 43,678 patients were diagnosed with cancer, and the crude incidence of any cancer was 500.6 per 100,000 personyears (95% CI, 495.9 to 505.3). The age-standardized incidence was calculated as 464.9 per 100,000 person-years. The most commonly diagnosed primary cancer among the sample was thyroid cancer (incidence, 64.3; 95% CI, 62.6 to 66.0), followed by stomach (incidence, 62.5; 95% CI, 60.8 to 64.2), colorectal (incidence, 59.8; 95% CI, 58.2 to 61.5), liver (incidence, 48.9; 95% CI, 47.5 to 50.4), and lung cancer (incidence, 48.0; 95% CI, 46.6 to 49.5). Among the male subjects, the top five incident cancers included stomach (incidence, 81.2; 95% CI, 78.5 to 83.9), colorectal (incidence, 67.1; 95% CI, 64.7 to 69.6), liver (incidence, 66.6; 95% CI, 64.2 to 69.0), lung (incidence, 64.3; 95% CI, 62.0 to 66.7), and prostate cancer (incidence, 63.2; 95% CI, 60.8 to 65.6), in that order. Thyroid cancer (incidence, 106.2; 95% CI, 103.2 to 109.3) was the most common cancer among the female subjects, followed by breast (incidence, 62.5; 95% CI, 60.2 to 64.9), colorectal (incidence, 52.5; 95% CI, 50.4 to 54.7), stomach (incidence, 43.8; 95% CI, 41.9 to 45.8), and lung cancer (incidence, 31.8; 95% CI, 30.2 to 33.5) (Table 2). The age-distribution of cancer incidence is illustrated in Fig. 2. The highest incidence was observed in the 70- to 79-year age group (incidence, 2,052; 95% CI, 2,002 to 2,104). The overall mean survival of cancer patients was 80.3±0.2 months from diagnosis, whereas the 5-year survival rate was 72.0±0.2% (Table 3).
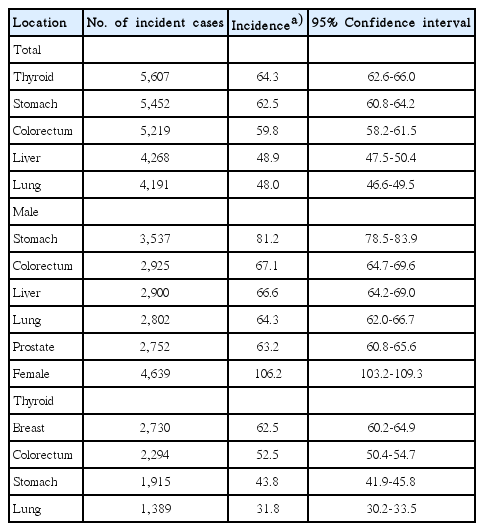
The five most common cancers in this cohort
Bar graph indicating the cancer incidence by age group. In general, older subjects show higher cancer incidence. The peak incidence is 2,052 per 100,000 person-years in subjects aged 70-79 years.
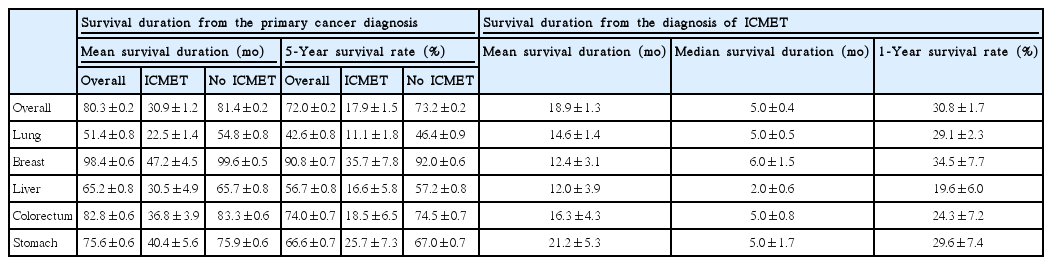
Survival features of the cancer patients in this cohort
A total of 776 subjects were diagnosed with ICMET. The crude incidence of ICMET was 8.9 per 100,000 person-years in the entire population (95% CI, 8.3 to 9.5). The age-standardized incidence of ICMET was 8.2 per 100,000 person-years. The mean interval between the date of the initial diagnosis of the primary cancer and ICMET was 13.1 months. Patients with ICMET survived for an average of 30.9±1.2 months from the date of diagnosis of the primary cancer, which was significantly shorter than that in patients without ICMET (81.4±0.2 months, p < 0.001). The 5-year survival rate was 17.9±1.5% in patients with ICMET and was 73.2±0.2% in cancer patients without ICMET. The mean survival duration from the date of ICMET diagnosis was 18.9±1.3 months (median, 5.0±0.4 months). Approximately 31% of the patients survived for > 1 year after ICMET diagnosis.
The incidence of ICMET among the cancer patients was 5.0 per 1,000 person-years (95% CI, 4.7 to 5.4). With regard to the number of cases, ICMET from lung cancer was found to be the most common metastasis type (n=417, 53.7%), followed by ICMET from liver (n=48, 6.2%), breast (n=46, 5.9%), and colorectal cancer (n=41, 5.3%) (Table 4).

Incidence and number of cases of ICMET based on the primary cancers
2. Lung cancer
With regard to the incidence of ICMET according to the primary cancer, lung cancer was found to be associated with the greatest ICMET incidence. Over the follow-up of 10,198 person-years among 4,191 subjects with lung cancer, 417 were diagnosed with ICMET. The incidence of ICMET was 40.9 per 1,000 person-years among lung cancer patients. The mean time interval between the primary cancer diagnosis and ICMET was 8.1±13.7 months. Moreover, the mean survival duration among lung cancer patients was 51.4±0.8 months from the date of the primary diagnosis; the 5-year survival rate was 42.6±0.8%. Among the subjects without ICMET, the mean survival duration was 54.8±0.8 months (5-year survival rate, 46.4±0.9%), which was significantly longer than that among subjects with ICMET (22.5±1.4 months, p < 0.001) (Fig. 3A). The 5-year survival rate was 11.1±1.8% in patients with ICMET. From the date of diagnosis of ICMET, these patients survived for an average of 14.6±1.4 months (median, 5.0±0.5 months) (Table 3).
Survival curves of lung (A), breast (B), and liver (C) cancer patients. Patients with intracranial metastases (ICMET) showed poorer survival (p < 0.001). The shading indicates the 95% confidence interval.
Cumulative incidence rate of ICMET from diagnosis of lung cancer was presented in Fig. 4. Among 417 ICMET from lung cancer, 178 (37.8%) were diagnosed simultaneously or prior to lung cancer. Thus, the slope of incidence curve was very steep at the origin. One-year cumulative incidence of ICMET was 8.8±0.5%. At 5-year observation, cumulative incidence reached to 13.6±0.7%.
Survival curve shows cumulative incidence of intracranial metastases (ICMET) from diagnosis of lung cancer. Initial steep slope indicates high rate of simultaneous diagnosis with primary cancer.
Incidence of ICMET from lung cancer patients was 44.2 and 35.6 per 1,000 person-years in male and female patients, respectively. In both sex, age group of peak incidence of ICMET was 60-69 years old. Incidence by sex and age was schematized in Fig. 5A. Survival of younger age group (< 60 years-old) was significantly better than older age group (p < 0.001). Median survival of younger and older age group was 8.0±1.4 months and 4.0±0.3 months, respectively. Regarding sex, female patients survived longer than male patients (median survival, 6.0±1.1 months vs. 4.0±0.5 months, p=0.007). Younger female patients showed best survival compared with older male patients (Fig. 5B).
(A) Bar graph shows detailed statistics of incidence by sex and age groups. (B) Survival function by sex and age group. Younger age group represents age < 60 patients. ICMET, intracranial metastases; Y/M, younger male; Y/F, younger female; O/M, older male; O/F, older female.
Chronological analysis for ICMET from lung cancer revealed that incidence of ICMET from lung cancer has been gradually increased with the years. It was 88.2 per 1,000 person-years in 2012 while it had been 17.5 per 1,000 person-years in 2005. Furthermore, interval between primary diagnosis and ICMET has been getting shorter from 11.8 months in 2005 to 5.3 months in 2012. Nevertheless, 1-year survival rate from diagnosis of lung cancer or ICMET has been consistent during observation period (Fig. 6).
Line graphs shows chronological change of statistics regarding intracranial metastases (ICMET) from lung cancer. Incidence shows incremental trend over years, while mean interval does descending.
3. Breast cancer
During the observation period, 46 patients were found to have developed ICMET from breast cancer; these patients represented 5.9% of all ICMET cases. Considering the observation size among the breast cancer patients (10,094 person-years), the incidence of ICMET among breast cancer patients was estimated as 4.2 per 1,000 patient-years, which was the second-highest value, after lung cancer. The mean time interval between the primary cancer diagnosis and ICMET diagnosis was 30.9±21.8 months. The overall mean survival of breast cancer patients from the date of the primary cancer diagnosis was 98.4±0.6 months, and the 5-year survival rate was 90.8±0.7%. Patients without ICMET survived for longer (99.6±0.5 months) than those with ICMET (47.2±4.5 months, p < 0.001) (Fig. 3B). The 5-year survival rate from the date of primary cancer diagnosis in patients without ICMET was 92.0±0.6%, and was 35.7±7.8% in patients with ICMET. The mean survival duration from the date of ICMET diagnosis was 12.4±3.1 months (median, 6.0±1.5 months). Approximately 35% of the patients survived for > 1 year after the diagnosis of ICMET, which was the highest value among the five most common ICMET-producing cancer cases.
4. Liver cancer
A total of 4,268 patients were diagnosed with liver cancer in this study. Among these patients, 48 were found to have developed ICMET after a mean interval of 17.6±19.9 months; these patients represented 6.2% of all ICMET patients. The incidence of ICMET among the liver cancer patients was 3.4 per 1,000 person-years. The 5-year survival was 56.7±0.8%, and the mean survival duration of liver cancer patients was 65.2±0.8 months from the date of the primary cancer diagnosis. The survival duration from the date of the primary cancer diagnosis was significantly shorter in patients with ICMET from liver cancer (30.5±4.9 months) than among those without ICMET (65.7±0.8 months, p < 0.001) (Fig. 3C). Moreover, the 5-year survival rate of patients with and without ICMET was 16.6±5.8% and 57.2±0.8%, respectively. Patients with ICMET from liver cancer showed the worst survival features. The mean survival duration from the date of ICMET diagnosis was 12.0±3.9 months (median, 2.0±0.6 months), and < 20% of patients survived for > 1 year (Table 3).
5. Colorectal cancer
The incidence of ICMET from colorectal cancer was 2.1 per 1,000 person-years. Although the number of ICMET cases (n=41, 5.3%) from colorectal cancer was fourth-highest among the different ICMET-producing primary cancers, the ranking of incidence reduced to sixth due to the presence of a large denominator, observation size (19,096 person-years). The mean time interval between the primary cancer diagnosis and ICMET was 21.0±17.8 months. The mean survival duration of colorectal cancer patients was 82.8±0.6 months, from the date of the primary cancer diagnosis. The 5-year survival rate was 74.0±0.7%. Among the subjects with ICMET, the mean survival duration was 36.8±3.9 months (5-year survival rate, 18.5±6.5%), which was significantly shorter than that among subjects without ICMET (83.3±0.6 months, p < 0.001). The 5-year survival rate of patients without ICMET was 74.5±0.7%. The mean survival duration from the date of diagnosis of ICMET was 16.3±4.3 months (median, 5.0±0.8 months).
6. Stomach cancer
Stomach cancer was the second-most frequent cancer among the Korean population, and was the most frequent cancer among male subjects. Cases of ICMET from stomach cancer represented 5.0% of all the ICMET patients. The incidence of ICMET from stomach cancer was 2.1 per 1,000 person-years. The mean interval from the date of the primary cancer diagnosis was 19.7±18.2 months. The mean survival duration from the date of stomach cancer diagnosis was 75.6±0.6 months, and the 5-year survival rate was 66.6±0.7%. The survival duration of patients with ICMET from stomach cancer was shorter (40.4±5.6 months) than that among non-ICMET patients (75.9±0.6 months, p < 0.001). The 5-year survival rate of patients without ICMET was 67.0±0.7% and was 25.7±7.3% among patients with ICMET. These patients had an average survival duration of 21.2±5.3 months from the date of diagnosis of ICMET (median, 5.0±1.7 months).
7. Prostate and thyroid cancer
Over the 11,953 person-years observation period among 2,753 prostate cancer patients, the incidence of ICEMT was found to be 1.2 per 1,000 person-years; these patients represented 1.8% of all ICMET cases. Moreover, 12 patients developed ICMET from thyroid cancer during the 20,099-person-year observation period (incidence, 0.6 per 1,000 person-years).
Discussion
In the present cohort study, the overall cancer incidence was found to be 500.6 per 100,000 person-years. Previous reports by the Korea central cancer registry described the cancer incidence as 445.7 per 100,000 person-years in 2013 [8]. As our cohort represented a random selection of 2% of the Korean population, potential selection bias could exist. Rather, one of the most important reasons for such overestimation was that the present cohort database was observed over 9 years, whereas the Korea central cancer registry included annual incident cases of cancer. Although the initial population structure of the cohort was similar to that of the national population, the proportion of older individuals may increase over time. Older age is one of the most powerful risk factors for cancer development. However, as the NHIS-NSC database originally included a categorized age variable, the exact age of the subject could not be determined. Hence, the adjustment for age over time could not be performed in the present analysis.
Metastatic tumor is the most common condition among the various intracranial malignant tumors [14]. In the present cohort study, the incidence of ICMET (8.9 per 100,000 person-years) was within the range reported in the other countries [2,3,5-7]. The incidence of ICMET was higher than that of all the primary central nervous system malignant tumors combined (8.2 per 100,000 person-years). Considering the national population of Korea (approximately 51 million), we estimate that the annual number of cases of ICMET may be 4,540 per year. The most common primary cancer associated with ICEMT is reported to be lung cancer. In fact, in the present study, lung cancer was found to be the primary cancer in > 50% of all cases of ICMET. The annual incidence of ICMET among the lung cancer patients was estimated as 2,440.
Although the occurrence of ICMET in cases with liver cancer is reportedly rare, ICMET arising from liver cancer was the second-most common type (6.2%) among all the ICMET cases in this cohort investigation, only secondary to lung cancer. In a previous Korean report, eight of 3,100 hepatocellular carcinoma patients (0.3%) were found to have developed ICMET between 1987 and 1991 [15], although subsequent studies in other Asian countries indicated a higher incidence rate (2.2%-7.0%) [16,17]. In the present study, among 4,268 liver cancer patients, a total of 48 patients were diagnosed with ICMET (1.1%). Considering the high incidence of hepatocellular carcinoma in Korea and prolonged survival of these patients, the number of patients with ICMET arising from liver cancer is expected to increase in the future [18]. Thus, the high incidence of ICMET is problematic, but the prognosis of cases of ICMET arising from liver cancer is even worse. Consistent with previous reports, the median survival of patients with ICMET was only 2 months, which was lowest among the types of cancer analyzed in the present study. Thus, we believe that patients with liver cancer should be carefully evaluated for ICMET based on the primary diagnosis. Moreover, appropriate guidelines for the screening of such cases should also be established.
The major limitations of the present cohort study are related to the nature of the NHIS-NSC. This database comprised claims data from healthcare institutions, without any reports regarding imaging or histologic examinations. Hence, we could not evaluate the primary cancer based on the histologic classification (e.g., small cell or non-small cell lung cancer). Moreover, the accuracy of the registered diagnostic code may represent another potential issue of this database. Although there is a possibility of errors in the registration of the diagnostic codes, an independent review agency (Health Insurance Review & Assessment Service) operated by the government reviewed the relevancy of all claims. As ICMET, and other primary cancers, are special diagnoses wherein patients receive guaranteed financial support from the NHIS, the proportion of misdiagnoses may be limited. Another limitation of the present study was the lack of treatment information, including chemotherapy, radiotherapy, and surgery. As diversely located cancers require various drugs at different doses, there may be too many codes for appropriately entering a query. Similarly, radiotherapy involves various doses of treatment with different fractionation values. Moreover, it was unclear whether the treatments were intended for the metastatic lesion. Hence, in the present study, the treatment administered for ICMET was not considered in the analysis. To overcome the limitations presented by the NHIS database, a tailored and detailed registry is mandatory to elucidate the efficacy of treatment for ICMET, because as described in the present study, the development of ICMET is one of the most important clinical factors influencing the survival of cancer patients.
To our knowledge, this is the first report to describe the epidemiology of ICMET in Korea using a national database. The age-standardized incidence of ICMET was found to be 8.2 per 100,000 person-years among the entire population in Korea. In particular, the incidence of ICMET among cancer patients was 5.0 per 1,000 person-years. Furthermore, the most common primary cancer among those who developed ICMET was lung cancer, followed by liver and breast cancer.
Notes
This study used NHIS-NSC data (NHIS-2016-2-260) made by National Health Insurance Service (NHIS). The authors declare no conflict of interest with NHIS.
Acknowledgements
We are grateful to Alboukadel Kassambara, PhD (Department of Biological Hematology, CHRU Montpellier, 34000 Montpellier, France) for providing us with the visualization library for survival function (survminer, https://github.com/kassambara/survminer).