Real-World Treatment Patterns among Patients with Advanced Gastric Cancer in South Korea
Article information
Abstract
Purpose
The purpose of this study was to understand patient treatment patterns, outcomes, and healthcare resource use in cases of metastatic and/or locally recurrent, unresectable gastric cancer (MGC) in South Korea.
Materials and Methods
Thirty physicians reviewed charts of eligible patients to collect de-identified data. Patients must have received platinum/fluoropyrimidine first-line therapy followed by second-line therapy or best supportive care, had no other primary cancer, and not participated in a clinical trial following MGC diagnosis. Data were summarized using descriptive statistics. Kaplan-Meier analysis was used to describe survival.
Results
Of 198 patients, 73.7% were male, 78.3% were diagnosed with MGC after age 55 (mean, 61.3 years), and 47.0% were current or former smokers. The majority of tumorswere located in the antrum/pylorus (51.5%). Metastatic sites most often occurred in the peritoneum (53.5%), lymph nodes (47.5%), and liver (38.9%). At diagnosis, the mean Charlson comorbidity indexwas 0.4 (standard deviation, 0.6). The most common comorbidities were chronic gastritis (22.7%) and cardiovascular disease (18.7%). Most patients (80.3%) received second-line treatment. Single-agent fluoropyrimidine was reported for 22.0% of patients, while 19.5% were treated with irinotecan and a fluoropyrimidine or platinum agent. The most common physician-reported symptoms during second-line treatment were nausea/vomiting (44.7%) and pain (11.3%), with antiemetics (44.7%), analgesics (36.5%), and nutritional support (11.3%) most often used as supportive care. Two-thirds of inpatient hospitalizations were for chemotherapy infusion. Outpatient hospitalization (31.6%) and visits to the oncologist (58.8%) were common among second-line patients.
Conclusion
Most patients received second-line treatment, although regimens varied. Understanding MGC patient characteristics and treatment patterns in South Korea will help address unmet needs.
Introduction
Gastric cancer is the fourth most common cancer worldwide and the second most common cause of cancer-related deaths [1,2]. The incidence of gastric cancer is highest in East Asian countries and in some parts of South America, while its occurrence is lower in North America and Africa [1,3]. South Korea has the highest incidence rate of gastric cancer (age standardized, male vs. female: 64.2 and 26.7 per 100,000). Globally, a high proportion of patients are diagnosed with late-stage disease, and 5-year survival rates are < 25% for these patients. Gastric cancer is the second most commonly diagnosed cancer in South Korea, with male and female mortality rates of 37.1 and 15.0 per 100,000, respectively. Risk increases with advancing age, history of Helicobacter pylori infection and cigarette smoking [2,3].
There is high unmet need in gastric cancer as there are few approved agents, and treatment practices vary widely among countries [1,2], particularly in the second-line treatment setting. There is also limited information available on gastric cancer patient characteristics, healthcare resource use and treatment patterns [1,2,4].
Therefore, this study was conducted to understand treatment patterns, patient outcomes, and healthcare resource use in South Korean patients with metastatic and/or locally recurrent, unresectable gastric cancer (MGC), including cancer of the stomach and gastroesophageal junction with adenocarcinoma histology.
Materials and Methods
This study is a retrospective analysis of de-identified patient-level data from medical charts collected via a physician-administered online chart review or face-to-face interviews with physicians who treated gastric cancer patients. Physicians selected at random from a panel of oncologists and referrals to the study by local contacts and elected to participate in the study provided de-identified patient-level data from a random sample of patient charts.
This study received Investigational Review Board (IRB) exemption from the Seoul National University Hospital and from the Western Institutional Review Board.
1. Data collection
Per protocol, each physician could provide information from up to 10 patient charts. Inclusion in the study was limited to adult patients (≥ 18 years) diagnosed with MGC, including cancer of the stomach or gastroesophageal junction with adenocarcinoma histology, on or after January 1, 2009 (until data collection began in 2013). Patients could have been diagnosed with an earlier stage gastric cancer before January 1, 2009. Eligible patients had no other primary malignant tumors and completed platinum/fluoropyrimidine (P/F) first-line therapy (with or without other drugs; e.g., therapy with trastuzumab) after MGC diagnosis. Upon completion of first-line therapy, eligible patients either went on to (1) second-line therapy or (2) best supportive care (BSC) only. Patients were not eligible if they participated in any clinical trials after MGC diagnosis.
The chart abstraction instrument was designed to collect information on physician and patient characteristics, treatment patterns by line of therapy, patient outcomes, and health care resource use. Comorbidities were also collected to allow reporting of patients’ Charlson comorbidity index (CCI). The CCI is a validated tool based on 17 comorbidities that is used to predict the risk of 1-year mortality [5].
2. Statistical analysis
Patient characteristics were compared between patients who received second-line therapy and those who received only BSC after first-line therapy. Chi-squared tests were used for comparisons of proportions, and Wilcoxon rank sum tests were used for comparisons of continuous variables. p-values of < 0.05 were considered statistically significant. All data were evaluated descriptively with univariate analysis using SAS ver. 9.3 (SAS Institute Inc., Cary, NC).
Kaplan-Meier analysis was used to describe survival and disease progression. Survival time was calculated from (1) the date of MGC diagnosis to the date of death for all patients, and (2) from the date of initiation of second-line therapy to the date of death for the cohort that received second-line therapy. Patients surviving at the time of data collection were censored at the date of last contact. Patients who were reported to have died, but for whom no dates of death were available, were recorded as having died on the date of last contact.
Rates of disease progression defined as discontinuing any agent in that line of therapy due to disease progression were calculated for each line of therapy. Duration of each line of therapy was defined as the number of days from the first to the last administration of any agent in that line of therapy. Patients with ongoing second-line and third-line therapy were excluded from the calculations of mean duration of second-line and third-line therapy, respectively, but not from Kaplan-Meier analyses of survival and disease progression.
Healthcare resource utilization, including inpatient and outpatient office visits, was calculated for each line of therapy. Observations were excluded from the calculation of each resource use category if it was unknown in what line of therapy they occurred.
Results
1. Physician characteristics
Thirty physicians that were selected at random from a panel of oncologists and referrals to the study by local contacts and elected to participate in the study provided de-identified patient-level data from 198 patient charts. Most physicians (27/30, 90%) specialized in gastric oncology, and the average time in practice was 11.5 years (standard deviation [SD], 5.5 years). Nine of 30 physicians reported affiliation with one of the major cancer centers in South Korea based on a limited set of centers noted in the survey instruments. Data were collected from February 20, 2013, to April 29, 2013. No data identifying the physicians were collected, and only physicians had access to the medical charts during the abstraction process.
2. Patient and disease characteristics
Charts were abstracted for 198 MGC patients. At MGC diagnosis, patients were 61.3 years old (SD, 9.8) on average, and 73.7% were male. Most patients (41.9%) had no history of smoking, while 19.2% and 27.8% were current or former smokers, respectively. Alcohol use was most frequently light to moderate (47.5%), although 9.1% of patients had a history of heavy alcohol consumption. A history of H. pylori infection or a family history of gastric cancer was observed in 4.0% and 6.6% of patients, respectively (Table 1).

Baseline patient and disease characteristics at diagnosis
The most commonly reported comorbidities were chronic atrophic gastritis (22.7%), cardiovascular disease (18.7%), intestinal metaplasia (14.1%), and diabetes without chronic complications (12.1%). Excluding malignancy and metastatic solid tumor diagnoses, the mean CCI was 0.4 (SD, 0.6) (Table 1).
3. Disease and tumor characteristics
Upon initial gastric cancer diagnosis, 76.8% of patients had stage IV disease according to the American Joint Committee on Cancer TNM (tumor size, lymph nodes affected, metastases) system [6]. At MGC diagnosis, 97.5% of patients had stage IV disease, with diffuse histology (by the Laurén system [7]) being the most frequently reported type (33.3%). There were no patients with stage III disease, and the staging for the remaining 2.5% of patients was unknown/other. Histology information was missing for 32.8% of patients. The antrum and pylorus were the primary tumor locations in the majority of patients (51.5%). The most frequently reported metastatic sites were the peritoneum (53.5%), lymph nodes (47.5%), and liver (38.9%) (Table 1). On average, MGC diagnosis occurred 4.5 months (SD, 14.3) after initial gastric cancer diagnosis.
Only 84 of the 198 patients were tested for HER2 positivity, of which 9.5% had positive status (Table 1). Variability in HER2 positivity rates of testing over a 5-year period including 2009 to 2013 ranged from 0% in 2009 to 52.0% in 2012, with an overall rate of testing of 42.4% for patients in this sample. A higher percentage of patients were tested for HER2 status at major cancer centers (68.0%) than patients treated in other centers (30.0%).
4. Treatment patterns
1) First-line therapy
By design, all patients in the study were required to have first-line therapy for MGC. At therapy initiation, most patients (76.3%) were symptomatic but completely ambulatory (Eastern Cooperative Oncology Group performance status [ECOG PS], 1), while some remained asymptomatic (ECOG PS, 0; 12.6%).
In this sample of 198 patient charts, the most frequent first-line regimen type was a fluoropyrimidine with a platinum agent (+/– leucovorin) (60.6%), which consisted primarily of 5-fluorouracil with a platinum agent (40.9%), capecitabine with a platinum agent (14.6%), or S-1 with a platinum agent (5.1%). Single-agent fluoropyrimidine (+/– leucovorin) was prescribed for 19.2% of patients, and in fewer patients, irinotecan plus platinum and/or fluoropyrimidine (+/– leucovorin) (4.5%) was prescribed (Table 2). For 88.9% of patients, physicians reported selecting first-line treatment based on national guidelines. For 22.7% of patients, physician experience was a factor in selection of the first-line treatment regimen.

Patient status and treatment regimens by line of therapy
First-line treatment lasted a median of 84 days (interquartile range [IQR], 49 to 155 days). Response to treatment included stable disease (52.0%), partial response (25.3%), disease progression (18.2%), complete response (3.0%), and unknown (1.5%). In 75.8% of patients, first-line therapy was discontinued due to disease progression, while it was discontinued in 12.6% of patients because of an adverse event (AE) or toxicity. Other reasons for discontinuation included patient preference, completion of protocol, lack of benefit, and unknown.
2) Second-line therapy and BSC
In this study, 39 patients (19.7%) received BSC only following first-line therapy, while 159 (80.3%) received second-line therapy.
Second-line therapy was initiated due to tumor progression in 95.6% of patients. When qualitatively compared with first-line regimens, second-line regimens were more heterogeneous. Physicians reported treating 22.0% of patients with a single agent fluoropyrimidine (+/– leucovorin), 19.5% with irinotecan with a platinum agent and/or fluoropyrimidine (+/– leucovorin), 13.2% with fluoropyrimidine with a platinum agent (+/– leucovorin), and 8.2% with single-agent taxane. Other types of regimens were used in 37.1% of patients (Table 2). For 80.5% of patients, physicians reported selecting second-line therapy based on national guidelines, while in 34.6%, selection was guided at least in part by experience.
Second-line treatment lasted a median of 64 days (IQR, 37 to 105 days). The most frequent best response to therapy was stable disease (45.9%). Partial response was observed in 15.1% of patients, complete response in 1.3%, progression occurred in 22.6%, and response was unknown for 15.1%. Second-line therapy was discontinued because of disease progression in 61.6% of patients, patient refusal in 17.6%, AEs or toxicity in 11.3%, lack of benefit in 2.5%, other in 1.3%, end of protocol in 0.6%, and for unknown reasons in 13.2% of patients. When we stratified patients between those who received BSC and those who received second-line therapy, we found differences only in age and ECOG PS. Patients who received second-line therapy after first-line treatment were younger and more likely to be asymptomatic (Table 3).

Patient demographic characteristics stratified by BSC or second-line therapy after first-line therapy
3) Third-line therapy
Third-line therapy was administered in 23.2% of patients (46 out of 198). Due to the small number of patients who received third-line therapy, treatment patterns were not evaluated in detail.
5. Physician-reported patient symptoms, supportive care, and healthcare resource use
For each line of therapy, physicians reported symptoms in patients related to either cancer or cancer treatments. The most common cancer-related symptoms or complications reported were pain in 26.3%, 27.7%, and 30.4%, and nausea/vomiting in 13.6%, 10.7%, and 10.9% of patients during first-, second-, and third-line therapy, respectively. Gastric obstruction was recorded in 5.6%, 6.3%, and 13.0%, ascites in 3.5%, 6.3%, and 6.5%, and bleeding in 3.0%, 1.9%, and 0% of patients undergoing first-, second-, and third-line therapy, respectively (Fig. 1).
Physician-reported symptoms (% of patients) by line of therapy. a)Other symptoms or complications included bruises, diarrhea, neuralgia, mucositis, weakness, fatigue, hand numbness, hand-foot reaction, dermatitis, varicella, weakness of whole body, and leukopenia.
Symptoms related to cancer treatment were similar to those recorded for cancer. Nausea/vomiting was reported in 43.9%, 44.7%, and 19.6%, pain in 10.6%, 11.3%, and 23.9%, and ascites in 0.5%, 2.5%, and 2.2% of patients undergoing first-, second-, and third-line therapies, respectively. Treatment-related symptoms were similar during second-line treatment, with nausea/vomiting (44.7%) and pain (11.3%) being the most common. Fewer than 1% of patients experienced gastric obstruction or bleeding during any line of treatment.
Supportive care needs were common during first-, second-, and third-line therapies as well as BSC, and most frequently consisted of antiemetics (52.0%, 44.7% and 45.7%, 17.9%), analgesics (37.4%, 36.5% and 28.3%, 23.1%), and granulocyte colony-stimulating factors (5.6%, 8.2% and 6.5%, 0%). Nutritional support was provided to 13.6%, 11.3% and 8.7% of patients undergoing first-, second-, and third-line treatment and 4% of patients during BSC (Table 4). The most commonly performed procedure was endoscopy, which was conducted in 18.2%, 7.5%, and 4.3% of patients during first-, second-, and third-line treatment, respectively, and in 10.3% of patients in BSC.
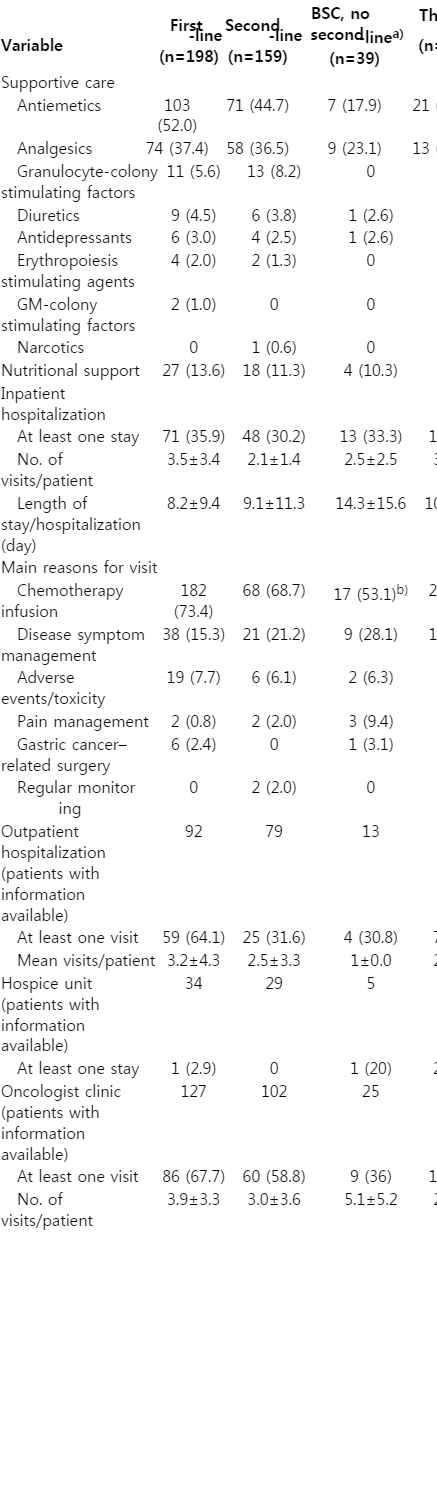
Patient supportive care and hospitalization stratified by line of therapy
Inpatient hospitalizations were reported in 35.9% of patients during first-line treatment, 33.3% of patients receiving BSC only, and 30.2% of patients during second-line treatment. Chemotherapy infusions and disease symptom management were the most commonly cited reasons for inpatient hospitalizations across all groups (Table 4).
Outpatient hospitalizations, which were most frequently for disease symptom management or AE/toxicity, occurred in 64.1% of patients during first-line treatment, 31.6% of patients in second-line treatment, 33.3% of patients during third-line treatment, and 30.8% of patients receiving BSC. Visits to oncology clinics, which were most commonly associated with pain management, were reported in 67.7%, 58.8%, 35.7%, and 36.0% of patients receiving first-, second-, and third-line treatment, and BSC, respectively (Table 4).
6. Survival and disease progression
Overall, the median survival time was 26.8 months (IQR, 9.9 to 41.6 months) from MGC diagnosis with 72.7% of patients censored. Patients who received second-line therapy had a median survival of 28.1 months (IQR, 10.5 to 36.6 months) with 74.2% of patients censored. Patients who received BSC only following first-line therapy had a median survival of 20.1 months (IQR, 8.5 to 41.6 months), with 66.7% of patients censored.
Among patients who received second-line therapy, median survival from initiation of second-line treatment was 13.0 months (IQR, 4.5 to 24.7 months) with 59.6% of patients censored.
Discussion
Our observational study supplements the information currently available regarding treatment of MGC in South Korea. We found variations in treatment patterns in both first- and second-line treatment regimens of patients with MGC. These findings are consistent with the results reported for a REGATE study in which 96% of patients received adjuvant chemotherapy consisting of varying agents, combinations and routes of administration [4]. Recently published guidelines for the diagnosis and treatment of gastric cancer in Korea [8] recommend fluoropyrimidines, platinums, taxanes, irinotecan, and anthracyclines as first-line chemotherapy and state no standard for second-line has been established, while these guidelines were published prior to recent approvals the second line [9-11]. In the present study, the selected patients were required to have P/F first-line therapy (with or without other drugs; i.e., therapy with trastuzumab) after MGC diagnosis, but these criteria were not strictly adhered to and impacted the treatment regimens observed during first-line therapy. Following first-line treatment, 80.3% of the studied patients received second-line treatment, while 19.7% of patients received BSC. The large proportion of patients receiving second-line treatment rather than BSC only may have been due to recent reports of the clinical benefits of second-line chemotherapy to overall survival and quality of life [12-14]. In the REAL-2 study, which was a randomized, controlled clinical trial, only 14% of patients received second-line treatment [15]. More recently, in the AVAGAST trial, 66% of Asian patients received second-line treatment [16]. Patients in our study were required to have had either second-line therapy or BSC after first-line therapy. These criteria may impact survival estimates following MGC diagnosis. Patients in our study who received second-line treatment were younger and had higher ECOG PS than those who received BSC. Performance status was reported to be a predictor of response to chemotherapy [17]. A recent meta-analysis suggests that patients with PS 0 have better survival after chemotherapy than those with PS 1 [18]. Among patients who received second-line therapy in the present study, 61.6% discontinued treatment because of disease progression and 46 patients (23.2%) received third-line treatment, highlighting the need for more clinical trials in advanced gastric cancer.
Overall, 42% of patients in this sample were tested for HER2 positivity, with a larger proportion of patients tested annually during the more recent years of the study. Of those tested, 9.5% tested positive for HER2. This rate of HER2 expression is consistent with the 6%-35% rate reported for gastric cancers [12,19]. HER2 testing is recommended in Korean gastric cancer treatment guidelines and in the ESMO and National Comprehensive Cancer Network guidelines [8,20,21]. Current guidelines recommend the addition of trastuzumab to chemotherapy in HER2+ patients [22].
Physician recommendations for MGC first-line therapy were most influenced by national guidelines and publications in top clinical journals. While the majority of first-line regimens administered to patients in this study consisted of a platinum agent and fluoropyrimidine as per eligibility criteria, second-line therapies varied widely, and include regimens that consisted of various single-agent fluoropyrimidines, doublet and triplet regimens, and single-agent taxanes. In a large, international prospective study of gastric cancer treatment (REGATE I), the use of a taxane such as paclitaxel, docetaxel, or irinotecan was reportedly the suggested second-line treatment for gastric cancer in Asia, though fewer than 10% of patients in the present sample were prescribed a taxane [1]. Other recent studies have reported a survival advantage associated with treatment with a second-line taxane such as docetaxel, or with irinotecan for cancers refractory to fluoropyrimidine and platinum treatment when compared to BSC [13,14]. In addition, no single agent option has been shown to be better than another in the second-line setting [18,23]. In our data, there appeared to be a trend in the increased use of taxanes as second-line therapy in 2012 relative to earlier years of the study (2009-2011); however, taxanes were prescribed to less than 20% of patients.
Best response to therapy and reasons for discontinuation of first- and second-line therapies revealed a significant unmet need in the treatment of MGC. Most patients achieved at most partial response or stable disease while on first-line therapy, and most discontinued this treatment due to disease progression. Similarly, the reason for initiating second-line therapy was tumor progression in 96% of patients. Responses to second-line therapy were less favorable than those to the first-line. In addition to disease progression, a major reason for discontinuing second-line therapy was patient refusal.
Healthcare resource use was driven both by chemotherapy administration and symptom management. The most commonly reported cancer treatment-related symptoms experienced by patients were nausea/vomiting and pain, and the most commonly used supportive care agents were antiemetics and analgesics. In addition to inpatient hospitalization visits for chemotherapy administration, patients were often seen in outpatient hospitals and oncology clinics for management of disease symptoms, AEs, toxicities, and pain.
It should be noted that this study is subject to the limitations of physician-administered chart abstractions. The completeness and accuracy of collected patient-level information depended on the accuracy of the physician recording the medical history information and treatment information, as well as the availability of a complete medical history in patient charts. Automated quality control checks for survey questions helped minimize possible inconsistencies in the recording of information. Patient-reported information documented in medical records and abstracted in this study may have been subject to self-report bias, including histories of smoking and alcohol use. Moreover, physicians may not have had full access to records documenting medical care administered to the patients over the course of MGC treatment, or to medical history prior to MGC diagnosis. Because a physician agreement was needed to participate, selection bias may play a role and treatment pattern information may not be representative of the treatment practice of all physicians or the treatments for all MGC patients in South Korea. It is important to interpret these results in light of the fact that the timeframe of this study was prior to more recent evidence supporting new therapies to guide practice in this space [9-11]. In addition, more than 70% of the study population was censored for survival, which is relatively high and may limit interpretation of the survival data.
Conclusion
The present study documents the high disease burden of gastric cancer and the significant unmet need that exists, particularly in the second-line setting. This study may help inform clinical practice and future research to ultimately improve patient outcomes.
Notes
This study was supported by Eli Lilly and Company. The following authors are employees of Eli Lilly and Company and may own company stock: G.C.C., A.M.L., N.R., R.C., and J.S.K.
Acknowledgements
The authors wish to thank the physicians who participated in the data collection for this study.