Predictors of Axillary Lymph Node Metastases (ALNM) in a Korean Population with T1-2 Breast Carcinoma: Triple Negative Breast Cancer has a High Incidence of ALNM Irrespective of the Tumor Size
Article information
Abstract
Purpose
We estimated the likelihood of breast cancer patients having axillary lymph node metastases (ALNM) based on a variety of clinical and pathologic factors.
Materials and Methods
Three hundred sixty-one breast cancer patients without distant metastases and who underwent breast conserving surgery and axillary lymph node dissection (ALND) (level I and II) or modified radical mastectomy (MRM) were identified, and we retrospectively reviewed their pathology records and treatment charts.
Results
Positive axillary lymph nodes were detected in 104 patients for an overall incidence of 28.8%: 2 patients (5%) with T1a tumor, 5 (9.2%) with T1b tumor, 24 (21.8%) with T1c tumor and 73 (44.2%) with T2 tumor. On the multivariate analysis, an increased tumor size (adjusted OR=11.87, p=0.02), the presence of lymphovascular invasion (adjusted OR=7.41, p<0.01), a triple negative profile (ER/PR-, Her2-) (adjusted OR=2.09, p=0.04) and a palpable mass at the time of diagnosis (adjusted OR=2.31, p=0.03) were all significant independent factors for positive ALNM.
Conclusion
In our study, the tumor size, the presence of lymphovascular invasion, a triple negative profile and a palpable mass were the independent predictive factors for ALNM. The tumor size was the strongest predictor of ALNM. Thus, the exact estimation of the extent of tumor is necessary for clinicians to optimize the patients' care. Patients with a triple negative profile have a high incidence of ALNM irrespective of the tumor size.
Introduction
Despite the advent of new tumor markers, axillary lymph node metastasis (ALNM) is still the most significant prognostic indicator for patients with invasive breast cancer (1-4). It is well known that a manual clinical examination of the axilla has poor sensitivity and specificity (5). Hence, a form of axillary nodal dissection is required to determine the axillary nodal status, and level I-II axillary dissection is considered the standard of care. Although no definitive evidence exists as to the therapeutic role of axillary lymph node dissection (ALND), it is universally acknowledged that staging the axilla is mandatory for planning the proper treatment of patients with invasive breast cancer (6,7). However, ALND has been shown to be associated with complications such as pain, lymphedema and shoulder stiffness (8).
Sentinel lymph node biopsy (SLNB) reduces the incidence of such complications and it is not associated with an increased risk of regional tumor recurrence. Thus, SLNB has been advocated for patients with T1-2 tumors and who have no clinically palpable axillary lymph nodes (9). For this reason, SLNB has been introduced in the last decade, and this procedure allows surgeons to avoid unnecessary axillary dissection in many cases. However, SLNB requires the talents of a multidisciplinary team that includes the surgeons, a nuclear medicine specialist, a radiologist and a pathologist, and this procedure prolongs the operative time. SLNB is a time-consuming procedure, and the frozen section evaluation has a 15~20% false negative rate that leads the patients to a second surgery and a significant increase in cost. In spite of these limitations, there is no question that SLNB is a worthy procedure.
If the axillary lymph node status could be accurately predicted prior to surgery, then selected patients who have an acceptably low probability of ALNM might avoid a full ALND and its associated morbidity. The purpose of this study was to estimate the likelihood of axillary lymph node involvement based on a variety of clinical and pathologic factors. With the improved accuracy of preoperatively predicting the axillary status, the patient care will be optimized by modifying the surgical, radiotherapeutic and chemotherapeutic strategies.
Materials and Methods
1. Patients
We conducted a review analysis of a prospective database of all the patients who were diagnosed with T1 and T2 invasive breast carcinomas and who were treated at St. Vincent's Hospital between January 2000 and May 2009. Institutional review board approval was obtained before the record review. A population of 453 patients was identified, and their pathology records and treatment charts were retrospectively reviewed for the information on the patient characteristics and the tumor characteristics. From this group of 453 patients, 361 patients without distant metastases and who underwent breast conserving surgery and ALND (level I and II) or modified radical mastectomy (MRM) were identified and these patients were evaluated in this study.
The clinical information included the patients' ages and the tumor palpability. A lymph node lesion was recorded as palpable if it could be felt by at least one examiner prior to being radiographically identified, and it was scored as non-palpable if the physical examination was recorded as negative, but it was discovered by mammography.
2. Tumor characteristics
The histopathologic characteristics we evaluated included the tumor size, the histologic grade (1-3), the presence of lymphatic or vascular channel invasion, the estrogen receptor (ER) and progesterone receptor (PR) statuses, the epidermal growth factor receptor 1 (EGFR) and human epidermal growth factor receptor 2 (Her2) expressions, the ER/PR/Her2 profile and the presence of tumor calcification. In this study, the patients' breast cancer was classified into four groups based on the immunohistochemial (IHC) profile of the ER/PR and Her2/neu expressions (positive and/or negative) and the groups are as follow
ER/PR+,Her2+=ER+/PR+,Her2+; ER+/PR-,Her2+; ER-/PR+, Her2+
ER/PR+,Her2-=ER+/PR+,Her2-; ER+/PR-,Her2-; ER-/PR+,Her2-
ER/PR-,Her2+=ER-/PR-,Her2+
ER/PR-,Her2-=ER-/PR-,Her2-
The tumor size was determined using the largest dimension of the invasive tumor component as measured in the gross pathologic specimen and this was categorized using the tumor-node-metastasis system of the American Joint Committee on Cancer (10): T1mic=1 mm or less, T1a=1.1 mm to 5.0 mm, T1b=5.1 to 10.0 mm, T1c= 10.1 to 20.0 mm and T2=20.1 to 50.0 mm. Because there were only four patients in this study with T1mic lesions, the T1mic lesions were grouped together with the T1a lesions. IHC analysis was performed on the formalin-fixed, paraffin-embedded breast cancer tissue specimens. The ER and PR analyses were based on an IHC assay, in which a report of 10% or greater of the cells that had nuclear staining for either ER or PR was defined as positive. IHC was performed with anti-ER (Thermo, clone: SP1, dilution: 1 : 100, Fremont, CA) and anti-PR (Thermo, clone: SP2, dilution: 1 : 100, Fremont, CA) and using an auto-staining system. The breast cancer tumors were classified as Her2-positive if they demonstrated Her2 gene amplification using the fluorescence in-situ hybridization (FISH) method, or they were scored as 3+ by the IHC method. We routinely used the IHC method. The intensity of the membrane staining was defined by a semiquantitative score (0 to 3+). The tumor staining was compared to the staining of the normal breast epithelium from the same patient as a negative control. For clinical purposes, 3+ staining, which was defined as uniform and intense membrane staining in more than 30% of the invasive breast cancer cells, was considered as overexpression. The PathVysion Her2/neu probe kit (Vysis Inc, Downers Grove, IL) was used for the FISH analysis in some cases. The number of chromosome 17 signals, the Her2/neu signals and the number of tumor nuclei scored were recorded for each case. The cases were interpreted as being amplified when the ratio of Her2/chromosome17 signals was equal or greater than 2.0. We defined node positive (+) as one or more histologically documented axillary lymph nodes.
3. Statistical analyses
Univariate analysis (the chi-square test or Fisher's exact test) was used to evaluate the relationship between the clinical and pathologic variables and the ALNM status. Unadjusted odds ratios (OR), 95% confidence intervals (CI) and p-values were all calculated. Multivariate logistic regression analysis was performed to evaluate the relationship between the clinical and pathologic variables and the ALNM status with adjusting for all other factors. The adjusted OR's, 95% CI's and p-values are presented. Statistical significance was evaluated at the 0.05 alpha level. All the tests were two-sided. Data analysis was performed with commercial statistical software (SPSS 12.0; SPSS Inc., Chicago, IL).
Results
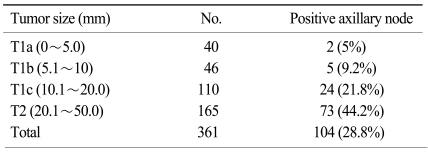
The patient and tumor characteristics, as stratified by the ALNM status, are presented in Table 1. There was a total of 361 patients, included 40 patients (11.1%) with T1a tumors, 46 (12.7%) with T1b tumors, 110 (30.5%) with T1c tumors and 165 (45.7%) with T2 tumors. The age of the patients ranged from 28 to 79 years with a mean age and median age of 50.1 years and 48.0 years, respectively. The mean number of lymph nodes examined per patient was 15.4±5.2 (mean±SD). As the tumor size increased, the frequency of positive axillary nodes also increased (Fig. 1). Positive axillary lymph nodes were detected in 104 patients for an overall incidence of 28.8%: 2 patients (5%) with T1a, 5 (9.2%) with T1b, 24 (21.8%) with T1c and 73 (44.2%) with T2. The frequency of the tumor subtypes according to the ER, PR and Her2 statuses are presented in Fig. 2, and the ER/PR+,Her2-profile was the most common subtype (n=189). The majority of the patients included in this study were Koreans (98%). Invasive ductal carcinoma was the predominant histologic type seen in 315 patients (87%), followed by medullary carcinoma in 20 patients (5%). There was no difference in the distribution of ALNM among the different histologic types.
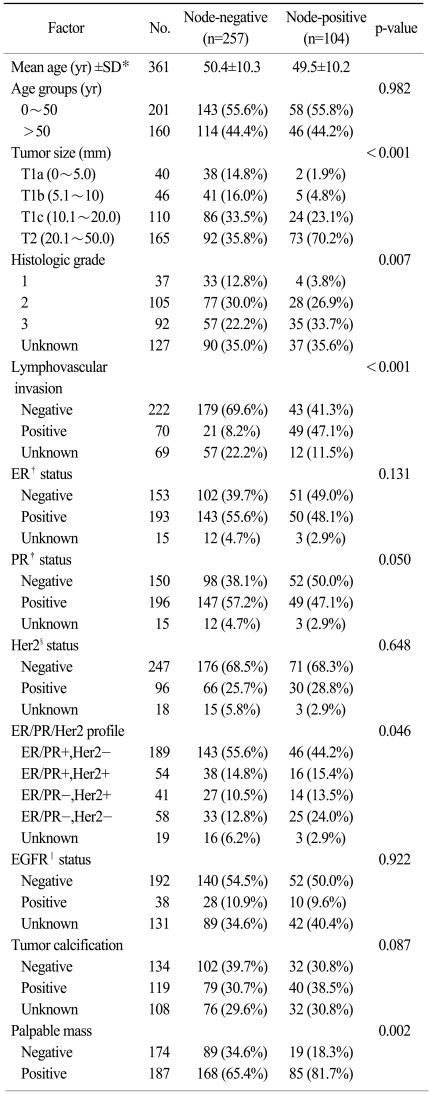
Patient and tumor characteristics (n=361)
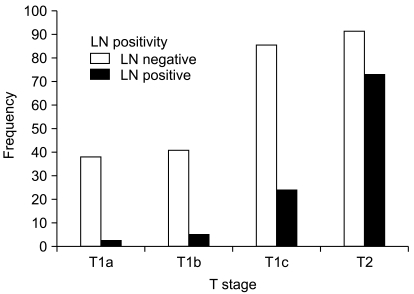
The frequency of nodal positivity according to the tumor size. Positive axillary lymph nodes were detected in 104 patients for an overall incidence of 28.8%: 2 patients (5%) with T1a; 5 (9.2%) with T1b; 24 (21.8%) with T1c; and 73 (44.2%) with T2. As the tumor size increased, the frequency of positive axillary nodes were also increased (p<0.001).
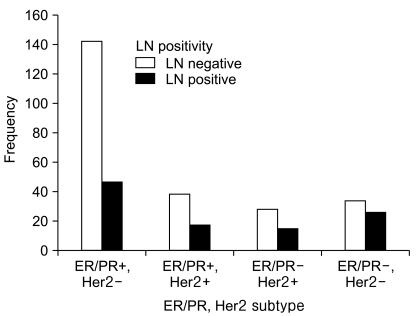
The frequency of the tumor subtypes according to the ER, PR and Her2 statuses. The ER/PR+,Her2- profile was the most common subtype (n=189). Patients with triple negative (ER/PR-,Her2-) profile have a significantly increased probability of ALNM than patients with ER/PR+,Her2- profile (p=0.006).
The univariate analysis for the relationship between the clinical and pathologic variables and the ALNM status is presented in Table 2. Six variables were found to be significant on the univariate analysis. These included an increased tumor size, a poor histologic grade, the presence of lymphovascular invasion, a PR-negative status, a triple negative (ER/PR-,Her2-) profile and a palpable mass at the time of diagnosis. Tumor size predicted nodal positivity and an increased tumor size was significantly associated with an increased risk of ALNM (OR=15.07, 95% CI: 3.52 to 64.56, p<0.001) (Table 3). A poorer histologic grade was significantly associated with nodal disease (OR=5.07, p=0.002). The presence of lymphovascular invasion was a significant factor for ALNM (OR=9.71, p<0.001), with 47.1% of the patients with ALNM having positive invasion compared with only 8.2% for the node-negative patients (p<0.001). PR-positivity was significantly associated with a negative status for ALNM (OR=0.63, p=0.05). The patients with a triple negative (ER/PR-,Her2-) profile had a more significantly increased probability of ALNM than the patients with an ER/PR+,Her2- profile (OR=2.36, p=0.006).
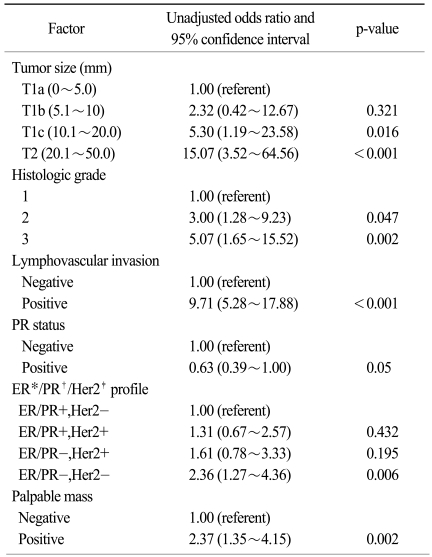
Univariate analysis of factors associated with axillary lymph node metastases
Tumor size and nodal positivity (p<0.01)
An additional multivariate logistic regression analysis was conducted on those variables that were found to be statistically significant on the univariate analysis. However, because of insufficient data we were unable to include the histologic grade and the PR status in the multivariate analysis. The relationships among the four clinical and pathological factors and the ALNM status are presented in Table 4. Again, an increased tumor size (adjusted OR=11.87, p=0.02), the presence of lymphovascular invasion (adjusted OR=7.41, p<0.01), a triple negative (ER/PR-,Her2-) profile (adjusted OR=2.09, p=0.04) and a palpable mass at the time of diagnosis (adjusted OR=2.31, p=0.03) were all significant independent factors for ALNM. We identified 17 patients who had 4 favorable clinical and pathologic parameters, which included a non-palpable mass at the time of diagnosis, T1a or T1b tumors, an ER/PR+,Her2+, ER/PR+,Her2+ or ER/PR-,Her2+ profile and a lack of lymphovascular invasion. When all the favorable factors were taken into account, none of the 17 patient (0%) had axillary lymph node involvement. On the contrary, a total of 12 patients were identified with all the unfavorable factors such as a palpable mass on diagnosis, T2 tumors, a triple negative (ER/PR-,Her2-) profile and the presence of lymphovascular invasion. Out of the twelve, 11 patients (91.6%) had axillary lymph node involvement.
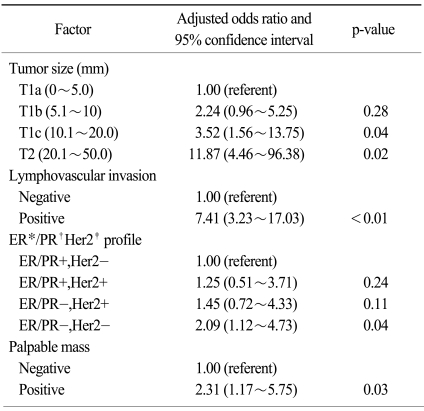
Multivariate analysis of factors associated with axillary lymph node metastases
Discussion
A common route of spread for breast carcinoma is first through the axillary lymph nodes, and the incidence of ALNM increases with larger tumors (11-14). Table 5 demonstrates the strong relationship between the primary tumor size and ALNM. Even patients with T1a and T1b disease have significant nodal involvement (5~15%). Similarly, the presence of lymphovascular invasion is a well known risk factor for ALNM, in accordance with a number of published studies (15-18). Using the most common subtype (ER/PR+,Her2-) as a reference, the patients with the triple negative (ER/PR-,Her2-) subtype has a significantly increased probability of ALNM (adjusted OR=2.09, p=0.04). Breast carcinomas have traditionally been classified as hormone receptor-positive or hormone receptor-negative. The newer approaches to breast carcinoma classification using the gene-expression profiles and IHC biomarkers have recently identified at least four subtypes (19). These subtypes are luminal A (ER/PR+,Her2-), luminal B (ER/PR+,Her2+), basal-like (ER/PR-,Her2-) and Her2-positive (ER/PR-,Her2+). The ER- and PR-negative tumors are generally thought to have a poor prognosis because they are not amendable to hormone therapy. Her2-negative tumors lack the benefit of Her2-targeted therapy and they are thought to have a worse prognosis. Onitilo et al. have recently shown that with using ER/ PR+,Her2- as a reference, the triple negative subtype has the worst overall survival and disease-free survival (20). In our study, for the patients with the ER/PR+,Her2- profile, the incidence of ALNM increased from 0% to 41.2% as the tumor got bigger. However, the patients with a triple negative profile had a high incidence (≥22.2%) of ALNM irrespective of the tumor size (Table 6). Non-palpable lesions lack the bulk that would make them palpable, so the number of tumor cells they contain may be less than that in a palpable tumor of equivalent diameter. Thus, there may be significant volume differences between equally sized palpable and non-palpable tumors. Those patients who undergo routine screening mammography are more likely to have their tumors diagnosed as non-palpable lesions, and these non-palpable tumors are more likely to be smaller and have lower nodal positivity. Silverstein MJ et al. demonstrated that tumor palpability was an independent predictor of ALNM on their multivariate analysis of more than 2,000 patients with breast carcinoma (12).
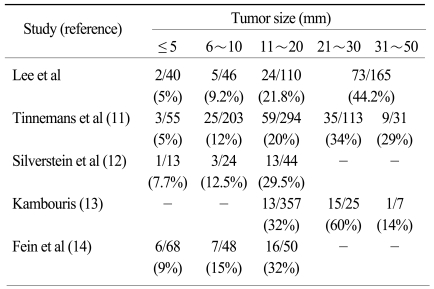
Incidence of axillary lymph node metastases in breast carcinomas
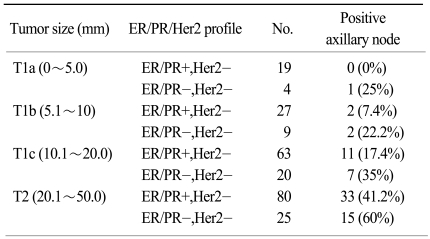
Nodal positivity according to tumor size and ER/PR/Her2 profile
Bader et al. reported that the primary tumor characteristics can be used to identify a subgroup of T1 breast cancer patients who have a low risk of ALNM. Preoperative risk assessment using the tumor grade, the tumor size, the presence of lymphovascular invasion and the Ki-67 staining might be used to omit routine ALND in those patients who are at a low risk for ALNM (21). In another study of lymph node metastases in relation to the histological type and clinical palpation, the investigators concluded that routine ALND could be omitted in those clinically node negative patients with stage T1a disease, a lymphovascular-negative tumor or a small tubular or mucinous carcinoma (<15 mm). However, dissection should be carried out for all the other cases, and it should be used as a therapeutic maneuver for most cases with palpable axillary lymph nodes (22).
A study is necessary to define the groups of patient who might or might not benefit from minimally invasive axillary staging such as SLNB and to determine whether or not SLNB, using both the dye and radionuclide techniques for maximum sensitivity and specificity, would be cost-effective. The extent of performing ALND remains controversial, and there has been fierce debate as to whether ALND is a staging procedure or a therapeutic procedure. Several prospective trials have shown no improvement in survival regardless of ALND, but there is an increased risk of axillary recurrence if no ALND is done (23). A full ALND is associated with some disabilities, i.e., lymphedema, shoulder stiffness and the loss of sensation of the inner arm. Hence, SLNB has become popular in the recent years, with several studies showing that there is no difference in survival or axillary recurrence when SLNB is compared to full ALND, and there is improvement in the quality of life (24).
On the univariate analysis, our study found that an increased tumor size, a poor histologic grade, the presence of lymphovascular invasion, a PR negative status, a triple negative (ER/PR-,Her2-) profile and a palpable mass found at the time of diagnosis were the significant factors for ALNM. On the multivariate analysis, an increasing tumor size, the presence of lymphovascular invasion, a triple negative (ER/PR-,Her2-) profile and a palpable mass at the time of diagnosis were the independent predictive factors for ALNM. This is similar to the findings of Harden et al., who found that vascular invasion and the tumor size were the independent predictive factors of positive nodes, but the tumor grade was not on the following multivariate analysis (25). Full axillary clearance of the lymph nodes should be carried out for the patients with T2 tumors as 44.2% of them will have nodal metastases. However, for the patients with T1 tumors and only a small percentage of whom (15.8%) have nodal metastases, a full axillary dissection would be over-treatment for almost 85% of these patients. For the T1 and T2 lesions, the difference in nodal positivity was statistically different for the palpable versus non-palpable lesions (p<0.05). For the patients with non-palpable T1 tumors, the incidence of nodal metastases was only 6.3%, whereas for those patients with palpable T1 tumors, the incidence of nodal metastases was 20.3% (Table 7). If a patient has a non-palpable T1 lesion, then less invasive axillay staging is strongly justified.
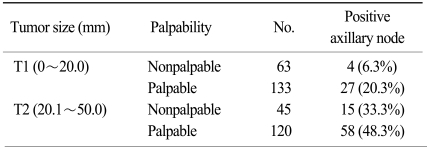
Nodal positivity according to tumor size and palpability (p<0.05)
Conclusion
We found that several of the patient characteristics and tumor characteristics such as the tumor size, the presence of lymphovascular invasion, a triple negative profile and a palpable mass are the independent factors to predict ALNM on the multivariate analysis for the patients who are diagnosed with T1 and T2 breast cancers. The tumor size is the strongest predictor of ALNM, so an exact estimation of the extent of tumor is necessary for clinicians to optimize the patients' care. The patients with a triple negative profile have a high incidence of ALNM irrespective of the tumor size. Thus, these patients need a form of axillary dissection for both the staging and treatment.