Introduction
Introduction of multiagent chemotherapy has resulted in significantly improved survival of patients with osteosarcoma [1,2]. However, improvements in survival have reached a plateau [3], and treatment outcomes for patients with metastasis or relapsed disease remain dismal [4-6]. Thus, novel agents that act via different mechanisms are needed in order to achieve further improvement in the survival rate [2,6].
Recent advances in molecular biology have resulted in identification of several pathways involved in the pathogenesis and progression of cancer. One of these is the epidermal growth factor receptor (EGFR) pathway, which is believed to be involved in progression of lung, colon, head, and neck cancers [7-10]. Following the success of gefitinib for treatment of non-small cell lung cancer [7,8], agents targeting EGFR via different mechanisms have been developed; some of these are currently undergoing clinical trials for treatment of colon, head, and neck cancers [10,11].
Although a large number of studies have been conducted for characterization of expression of growth factor receptors in bone and soft tissue tumors [12-14], the roles played by EGFR family members in osteosarcoma remain elusive. In vitro studies have reported expression of EGFR in osteosarcoma cells as well as effective inhibition of growth of osteosarcoma cells by EGFR inhibitors [15-17]. Expression of EGFR has been reported in 40-81% of osteosarcoma tumor tissues [13,14,17], however, its association with prognosis has been controversial. In one study, expression of EGFR showed an association with shorter overall survival (OS) of patients with osteosarcoma [17], while others have reported an association of its expression with good clinical outcome [18]. Furthermore, most of these studies analyzed Euro-American cases, and data on expression of EGFR in Asian patients with osteosarcoma is rare.
In the present study, we conducted a retrospective analysis of EGFR protein expression in osteosarcoma tumor samples obtained from Korean patients and examined associations between its expression and clinical features and treatment outcomes. In addition, in vitro studies were performed for evaluation of the efficacy of EGFR inhibitors, gefitinib and BIBW2992, on proliferation of osteosarcoma cells.
Materials and Methods
1. Patients and treatment
Thirty patients with primary osteosarcoma, treated at the Korea Cancer Center Hospital between 1995 and 2007 were retrospectively analyzed. The study was approved by the Institutional Review Board of Korea Cancer Center Hospital. Patients met the following criteria: 1) high-grade osteosarcoma; 2) no distant metastasis at the time of diagnosis; 3) no history of previous treatment; and 4) the availability of an incisional biopsy specimen taken prior to chemotherapy. A detailed summary of patient information is shown in Table 1. Treatments were dependent on concurrent medical problems. Two patients (case numbers 29 and 30) underwent surgery only, whereas the remaining 28 patients underwent two courses of preoperative chemotherapy followed by four courses of postoperative chemotherapy. Details regarding treatment have been previously described [19].
2. Immunohistochemical staining
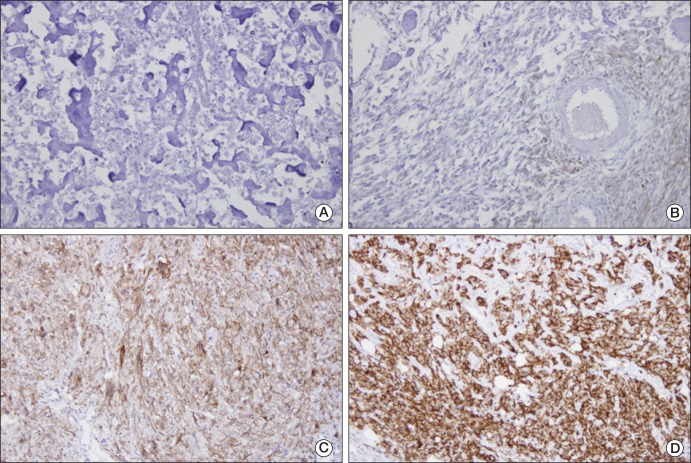
Representative areas, without spontaneous necrosis, were selected from incisional biopsy samples. We used a Zymed nonbiotin amplification system (Zymed Laboratories, South San Francisco, CA). Primary goat anti-human EGFR polyclonal anti-body and anti-goat EGFR biotinylated secondary antibody were purchased from Santa Cruz Biotechnology (Santa Cruz, CA). EGFR immunoreactivity was observed in membranes or cytoplasm of osteosarcoma cells. Some tissues showed strong immunoreactivity for EGFR, whereas others showed moderate or no immunoreactivity. Staining intensity was interpreted as follows: low, positivity of <10% of tumor cells; intermediate, positivity of 10-50% of tumor cells; and high, positivity of >50% of tumor cells.
3. Cell proliferation assays
Human osteosarcoma cell lines HOS, KHOS/NP, MG-63, and U-2 OS were obtained from the American Type Culture Collection (ATCC; Manassas, VA). Gefitinib and BIBW2992 were purchased from SelleckChem (S1025, S1011, Houston, TX), dissolved in dimethyl sulfoxide, and stored at -20℃. In each well of 96-well plates, 5,000 cells in 50 µL of media were seeded and incubated overnight at 37℃ in a humidified 5% CO2 incubator. On the following day, gefitinib and BIBW 2992 (0.01-20 µM) were added to wells and plates, followed by incubation for an additional 72 hours. A 3-(4, 5-dimethylthiazol-2-yl)-2, 5-diphenyltetrazolium bromide (MTT) assay was used for measurement of cell proliferation. IC50 values were determined from dose-response curves.
4. Western blot analysis
Cell lysates were prepared using a kit from Cell Signaling Technology (Beverly, MA). Equal amounts of protein (determined using the Bio-Rad Protein assay, Bio-Rad, Hercules, CA) were run on 12% sodium dodecyl sulfate polyacrylamide gel electrophoresis gels and transferred to polyvinylidene fluoride membranes, which were washed with Tris-buffered saline (TBS) containing 0.1% Tween 20 (TTBS), blocked with TTBS and 5% wt/vol nonfat dry milk overnight at 4℃, and incubated with primary antibody at 1 : 1,000 dilution. Membranes were then washed with TTBS, followed by incubation with horseradish peroxidase-conjugated secondary antibody (1 : 1,000). Signals were detected using an Amersham ECL (GE Healthcare Life Sciences, Munich, Germany).
5. EGFR mutation analysis
The genomic DNAs of the four osteosarcoma cell lines were extracted using a High Pure PCR template Preparation kit (Roche, Mannheim, Germany). PCR and real-time amplification monitoring of peptide nucleic acid PCR clamping were performed using a CFX 96 system (Bio-Rad). Genomic PCR was performed in final volume DNA and 0.75 U Taq polymerase (Solgent, Daejeon, Korea). The following sequencing primers were employed: E18-SF, 5-AGGTGACCCTTGTCTCTGTG-3, E18-SR, and 5-CCTGTGCCAGGGACCTTAC-3 for exon 18; E19-SF, 5-CATGTGGCACCATCTCACAA-3, E19-SR, and 5-CCCACA CAGCAAAGCAGAA-3 for exon 19; E20-B-F, 5-ATCGCATTCATGCGTCTTC-3, E20-B-R, and 5-GTCTTTGTGTTCCCGGACAT-3 for exon 20; E21-B-F, 5-CCTCACAGCAGGGTCTTCTC-3, E21-BR, and 5-GGAAAATGCTGGCTGACCTA-3 for exon 21. Sequences were compared with the GenBank-archived sequence of human EGFR.
6. Gene expression analysis
A Low Input Quick Amp labeling kit (Agilent Technologies, Santa Clara, CA) was used for labeling and amplification of total RNA samples (200 ηg), and Cy3-labeled amplified RNAs (aRNA) were re-suspended in 50 µL of hybridization solution (Agilent Technologies). Labeled aRNAs were then placed on an Agilent SurePrint G3 Human GE 8×60K array (Agilent Technologies) and covered with a Gasket 8-plex slide (Agilent Technologies). The slides were hybridized for 17 hours at 65℃, washed in 2× saline sodium citrate (SSC) containing 0.1% sodium dodecyl sulfate for 2 minutes, 1×SSC for 3 minutes, and then in 0.2×SSC for 2 minutes at room temperature, followed by centrifugation at 1,800× g for 20 seconds for drying. An Agilent scanner and its on-board software were used for analysis of arrays. Feature Extraction v10.7.3.1 (Agilent Technologies) was used for calculation of gene expression levels, and the Robust Multi-Array Average algorithm was used for generation of relative signal intensities for each gene. The quantile normalization method in GeneSpring GX 11.5.1 (Agilent Technologies) was used for processing of data.
7. Statistical analysis
The chi-square test was used for analysis of correlations between categorical clinicopathologic variables and EGFR expression. Variables analyzed included age, sex, tumor location, histologic subtype, tumor volume, and histologic response to preoperative chemotherapy. Tumor volumes were calculated using the ellipsoid formula [V = (4π/3)abc, where a, b, and c represent length, width, and depth] [19]. Kaplan-Meier survival analysis was used to examine relations between clinicopathologic variables and events (defined as either local recurrence, metastasis, or death). The log-rank test was used for calculation of survival differences according to clinicopathologic variables. SPSS ver. 11.5 (SPSS Inc., Chicago, IL) was used in performance of all calculations, and p-values of <0.05 were considered significant.
Results
1. EGFR protein expression, clinicopathologic characteristics, and outcome
Twenty-seven (90.0%) biopsy samples showed positive staining for EGFR protein (Table 1, Fig. 1); staining intensities for EGFR protein were as follows: high in 9, intermediate in 12, and low in 6. Neither the presence of EGFR staining nor its intensity showed an association with age, sex, tumor location, or histologic response to preoperative chemotherapy (Table 2). However, intermediate or high staining intensity for EGFR was related to a smaller tumor volume (p<0.001) and a histologic subtype other than osteoblastic type (p=0.03).
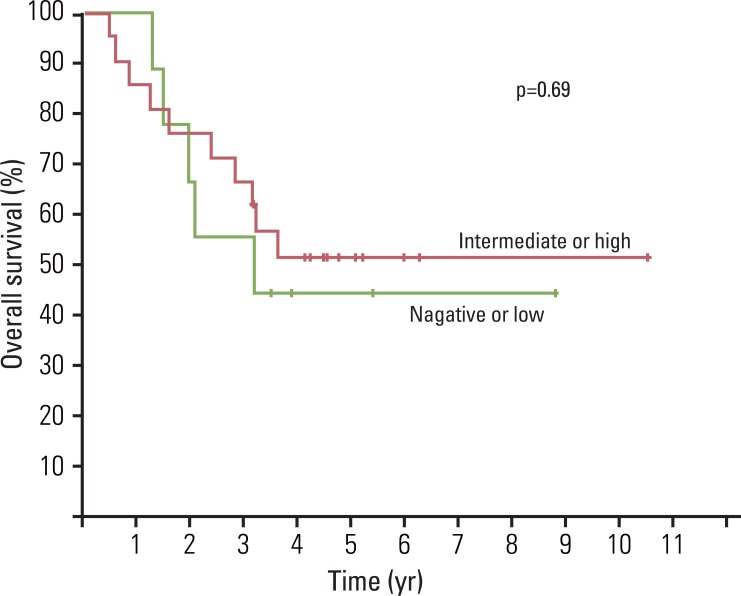
In addition, EGFR positivity and its staining intensity did not appear to be related to the survival (Fig. 2). Five-year OS for our 30 patients was 49.2±9.3%. Patients were followed for a median of 40.4 months (range, 6.0 to 126.0 months), and there were 17 events (14 distant metastases, 1 local recurrence, and 2 local recurrences combined with distant metastasis). Metastatic sites were as follows: lung (n=9), bone (n=3), lung and bone (n=3), adrenal gland (n=1), and pancreas (n=1). Median event-free survival for the 17 patients who experienced an adverse event was 9.3 months (range, 2.0 to 40.4 months).
2. Effect of EGFR inhibitors on the viabilities of osteosarcoma cell lines
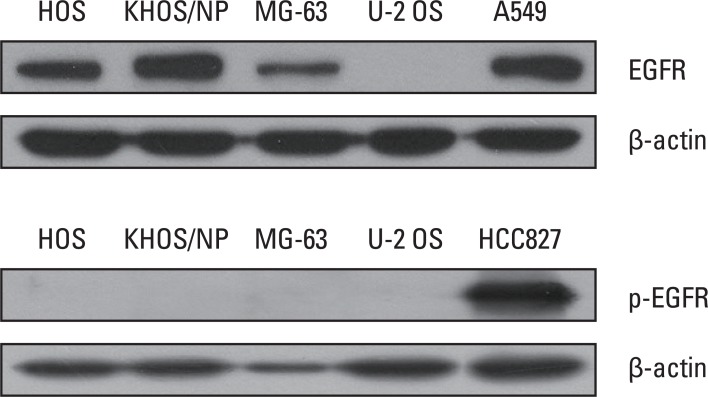
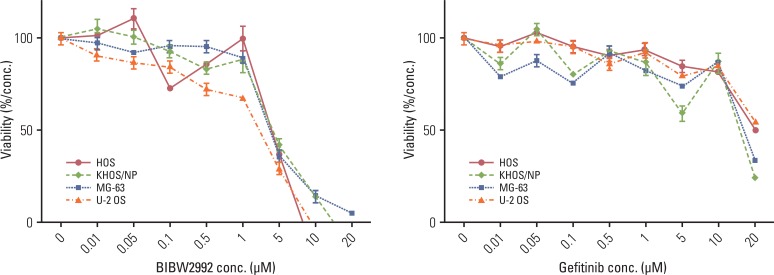
For the four osteosarcoma cell lines tested, expression of EGFR protein was observed in HOS, MG-63, and KHOS/NP cells, however, expression of p-EGFR was not observed in any cell line under basal culture conditions (Fig. 3). Osteosarcoma cells were exposed to gefitinib or BIBW2992 at concentrations ranging from 0 to 20 µM for 72 hours. However, no dose-dependent inhibitory effect was observed in any of the cell lines (Fig. 4).
3. Gene expression and mutation analysis of osteosarcoma cell lines
Table 3 shows expression of EGFR and phosphatase and tensin homolog (PTEN) in osteosarcoma cell lines. Expression of EGFR was observed at higher levels and its level of expression showed concurrence with western blot findings. However, PTEN was expressed at lower levels.
In the meantime, the tyrosine kinase domain from exons 18 to 21 was sequenced in all four cell lines, in order to determine whether they harbor constitutively activating mutations that confer sensitivity to tyrosine kinase inhibitors. We found single base changes at codon 2361 in exon 20 in HOS, MG-63, and KHOS/NP cells (G to A). However, these changes did not result in amino acid changes. Furthermore, we failed to find any known mutation associated with constitutive activation of EGFR in any of the four cell lines.
Discussion
In the present study, we found that EGFR protein is frequently expressed in osteosarcoma biopsy samples and cell lines. However, we found no association between expression of EGFR protein and treatment outcome, and, in addition, EGFR inhibitors gefitinib and BIBW2992 had no significant inhibitory effect on the viabilities of osteosarcoma cells. A single nucleotide change in the EGFR tyrosine kinase domain was identified by mutation analysis in all four osteosarcoma cell lines examined, however, no activating mutation was found.
Some limitations of the present study must be considered. First, due to the retrospective nature of this study, our study cohort included only a small number of patients who were treated over two decades. Thus, patients were not prospectively randomized and treatments were heterogeneous. Second, we believe that selection bias must have existed; for example, inclusion of patients who are older than 40 years. And the poor survival might have masked the prognostic significance of EGFR expression. Third, the reliance on immunohistochemistry and semiquantitative measures used for assessment of EGFR expression imposes limitations. Forth, although EGFR mutation status should have been determined in biopsy samples, due to the small sample sizes, it was limited to the four cell lines.
Relations between EGFR expression and the clinicopathologic characteristics of osteosarcoma remain elusive. In previous studies, involvement of EGFR in progression of lung, colon, head, and neck cancers has been suggested [7-11,20]. Thus, we supposed that EGFR expression might be related to the aggressive characteristics and poor treatment outcome of osteosarcoma. However, we found no relation between EGFR expression and treatment outcome; actually, an association with a small tumor volume was observed, which was not expected. We believe that this finding was probably due to the small sample size and section bias, however, it may be that the role of EGFR in osteosarcoma differs from that in adult carcinomas. Little data are available on the association between EGFR expression and clinical outcome in osteosarcoma. Freeman et al. [16] also failed to detect any association between EGFR expression and clinical findings in osteosarcoma, however, Kersting et al. [18] concluded that EGFR expression has a dose-dependent association with better prognosis in patients with high-grade osteosarcoma. Conduct of additional studies to elucidate the mechanism responsible for EGFR expression and for the clinicopathologic characteristics of osteosarcoma will be needed.
Contrary to our expectation, we observed no inhibitory effect of gefitinib and BIBW2992 on the viabilities of osteosarcoma cells. In order for EGFR-directed therapy to be available in osteosarcoma, assessment of its activation status and impact of its signaling on cell proliferation as well as the relationship between its expression and outcome need to be clarified. It has previously been suggested that osteosarcoma might be biologically dependent on EGFR-modulated cell signaling pathways [12,13,15,21,22]. Although expression of EGFR protein was observed in the four osteosarcoma cell lines that we tested, none of them expressed p-EGFR. It has been suggested that neither the expression level nor the phosphorylation status of EGFR showed correlation with sensitivity to gefitinib [23]. Although we tested gefitinib and BIBW2992 at different concentrations, we failed to observe any significant inhibitory effect on cell viability. The mutational status of EGFR has been reported to modulate responsiveness to EGFR inhibitors [9,24], therefore, we analyzed the tyrosine kinase domain of EGFR in the four osteosarcoma cell lines. Although an EGFR polymorphism was found in exon 20, it did not result in an amino acid change. In addition, we did not identify any activating mutation known to confer susceptibility to EGFR inhibitors. The osteosarcoma cell lines used in the present study exhibited slightly lower PTEN expression, loss of which is associated with resistance to anti-EGFR tyrosine kinase inhibitors [9,24]. The possibility exists that the lack of EGFR mutation and efficacy of EGFR inhibitors might be related to the cells we used. The cell lines analyzed were not of early passages, but were of multiple passages that might have accumulated many changes that were not present in the primary tumor specimens. Or, other EGFR-directed treatment modalities might be effective in osteosarcoma. Recently it was reported that anti-EGFR antibody cetuximab enhances the cytolytic activity of natural killer cell toward osteosarcoma cells [25]. Available data suggest the probable existence of subtle interplay between different growth factor receptors and downstream molecules in osteosarcoma. Conduct of further studies to elucidate the roles of EGFR and its inhibitors in osteosarcoma will be needed.
Conclusion
We found that EGFR protein is frequently expressed in osteosarcoma, however, this expression showed no association with treatment outcome. In addition, the two EGFR inhibitors, gefitinib and BIBW2992, had no observable inhibitory effect on viability of osteosarcoma cells, and mutation analysis of the EGFR tyrosine kinase domain failed to identify any activating mutation. However, considering that our study was performed using a limited number of biopsy samples and cell lines, and evaluated two kinds of EGFR inhibitors, conduct of further studies to explore the potential of other therapeutic agents targeting EGFR will be necessary.