Introduction
Oligometastasis (OM) was suggested by Hellman and Weichselbaum in 1995 [1] as a disease status in which the facility for metastatic growth is not fully developed and the numbers of metastases and the affected organ sites are limited. Hellman’s suggestion was based on the evidence showing that ablative local therapies for metastasis from various primary tumors resulted in extended survival or even curation in some patients [1–5]. After the introduction of this concept, the roles of metastasis-directed ablative local therapies of metastases from various primary tumors have been evaluated in numerous studies showing the benefits of metastasis-directed ablative local therapies in the improvement of survival outcomes [6–8]. However, the definitions and criteria of OM are diverse among the studies, especially in the number of metastases or affected organ sites, and has not been standardized, yet [9,10]. Therefore, the efforts to achieve the consensus have been made among the clinicians [11,12]. In the development of OM concept, data from early studies dealing with colorectal cancer (CRC) were utilized as evidence and current strategies recommended in the treatment of metastatic CRC (mCRC) depend on this concept [3,4].
It was reported that, in 2020, CRC accounted for 10% of the global cancer incidence, which was ranked in the third place following breast cancer and lung cancer and 9.4% of all cancer deaths, which was ranked in the second place following lung cancer [13]. Among the patients with CRC, 22% have initially diagnosed as stage IV CRC [14]. While the rates of distant metastasis in patients with stage I–II CRC are as low as at most 20%, 25%–50% of stage III patients may experience distant metastasis (including lymph node metastasis) later, which could be reduced in the range of 25%–30% following complete surgical resection plus subsequent adjuvant chemotherapy [15]. Although the survival time for patients with mCRC has been significantly extended over time, the reported 5-year overall survival (OS) rate remained < 20% [16]. The advances in various treatment strategies, including systemic therapy and local treatment for primary and metastatic disease, have contributed to the increased survival outcomes in the patients with mCRC. Especially, after the introduction of OM concept, metastasis-directed local ablative therapies have widely been utilized for hepatic or lung metastasis and resulted in the improved outcomes through successful local control (LC).
The liver is the most common site of distant metastasis in the CRC patients, which is related with the portal circulation, and accounts for approximately 25%–30% [17,18]. Although systemic treatment has played a critical role in metastatic setting, surgical resection of hepatic OM from CRC (HOCRC) has been recommended for the selected resectable cases which resulted in the improved 5-year OS rates upto 47%–60% [19–21]. However, only 15%–25% of HOCRC patients are eligible for resection due to the tumor or patient factors [22,23]. Therefore, alternative local ablative therapies were required to treat the HOCRC patients who are unsuitable for surgical resection. In the current guidelines for mCRC, various liver metastasis-directed local ablative therapies other than resection are listed that include radiofrequency ablation (RFA), microwave ablation (MWA), stereotactic ablative body radiotherapy (SABR), and embolization techniques [5,24].
Liver-directed local radiation therapy (RT) used to be regarded as unsafe, in the past, due to the fear of the risk for radiation-induced liver disease (RILD). Recent advances in RT technology during the last decade, however, have enabled highly precise and accurate liver-directed high-dose irradiation, and extended the use of new RT techniques in treating the HOCRC patients. In the previous prospective studies, the outcomes following SABR for liver metastasis from various primary sites showed high 2-year LC rate over 90% [25,26]. Furthermore, in the recent trials, SABR has improved the survival outcomes when compared with the standard of care for OM from various primary cancers, and the use of SABR for ablation of HOCRC is expected to increase. No randomized controlled trial comparing SABR with other modalities, however, has been performed yet, and the optimal regimen of SABR for HOCRC needs to be established.
Herein, the literature regarding curative local therapies for HOCRC is reviewed, and the role of SABR is discussed from the radiation oncologist’s and surgeon’s perspective. In addition, the future potential of SABR for treating the HOCRC patients is suggested.
Surgical Resection of HOCRC
Historically, curative resection was first attempted in the 1900s, and the relevant results from small series were reported. However, in the 1980s, a large amount of data from 24 institutions was published by Hughes et al. [3], which reported that curative resection in 607 HOCRC patients resulted in a 5-year disease-free survival (DFS) rate of 25%. These data supported the Hellman’s suggestion for the OM concept together with other series regarding pulmonary metastasectomy in sarcoma and renal cell cancer patients [1]. Subsequent large series on HOCRC endorsed the initial publication [27]. In a multicenter study by Pawlik et al. [28], a significantly improved 5-year OS rate of 58% was reported, when compared with the previous study. In particular, the researchers reported a significant association of negative resection margin with improved survival rate [28]. Recently, Bogach et al. [29] evaluated the outcome of resection of HOCRC at the population level, including 1,168 patients in the province of Ontario, Canada, from 2006 to 2015. They reported that the proportion of the patients who underwent resection increased 3% per year on average, and staged resection was more frequent than simultaneous resection (62% vs. 38%). The 5-year OS rate was 48% in the total population, and those who underwent simultaneous resection, when compared with staged resection patients, were associated significantly with shorter hospital stay (8 days vs. 11 days, p < 0.001), less frequent major resection (17% vs. 65%, p < 0.001), higher 90-day mortality (6% vs. 1%, p < 0.001), shorter median survival (40 months vs. 78 months, p < 0.001), and lower OS rate at 5 years (37.2% vs. 54.8%, p < 0.001), respectively. In various studies, long-term survival was also consistently reported. In Table 1, the relevant information of the selected studies is summarized. The improved OS rates following resection of HOCRC were not the only important findings in these studies. Various prognostic factors, including the number of hepatic tumors, size of hepatic metastasis, margin status after hepatic resection, disease-free interval, extrahepatic disease, disease burden of primary tumor, and tumor marker level, were also identified [30,31]. These parameters formed the basis of the OM concept, which were considered in the criteria and goals of resection of HOCRC. However, the consensus and eligibility criteria for resection of HOCRC have not established yet. Specifically, because the eligibility for surgical resection mainly depends on the estimated remnant liver volume following resection, underlying liver functional status, and location of metastatic tumor, only a small portion of the HOCRC patients is amenable to this approach. The surgical resection, however, has been extended along with a few new approaches: conversion therapy, which can shrink the tumor size and potentially convert from unresectable to resectable status; extending resection to extrahepatic disease; two-stage hepatectomy; and portal vein embolization inducing hypertrophy of the future liver remnant. Furthermore, the outcome of surgical resection of HOCRC could be improved by perioperative administration of chemotherapy [32]. However, there is a high percentage of HOCRC patients in whom complete LC could be attempted but surgery is not regarded a viable option. Therefore, alternative and supplementary methods to surgical resection are required, which include RFA, MWA, and SABR.
Radiofrequency Ablation for Hepatic Oligometastasis
RFA is the most commonly used local ablative approach. RFA can be conducted percutaneously or intraoperatively by placing the ablation electrodes in or around the tumor creating a thermal necrosis zone within the tumor and adjacent area [35]. RFA has shown up to 95% tumor response rates and safety in selected HOCRC patients who are not candidates for surgical resection [35,36].
Following RFA, excellent LC rate has been reported. In a randomized controlled trial, aggressive local treatments using RFA with or without surgical resection in addition to systemic treatment resulted in prolonged OS when compared with systemic treatment alone [37], which has made RFA a valid local ablative modality for HOCRC. However, when compared with surgical resection, RFA showed inferior outcomes. In a prospective randomized controlled trial, in the HOCRC patients with low tumor burdens and amenability to surgery, the outcomes following RFA and surgical resection, as the first-line treatment, were compared. This trial reported the local recurrence rates of 32% and 4% at the site of ablation and resection, respectively (p < 0.001) [38]. Several previous studies compared RFA and surgical resection (Table 2), which showed generally inferior LC and OS rates following RFA [27–36]. Kron et al. [39] performed a systematic review of 18 published studies and reported that among the studies, 10 and eight showed significantly higher local recurrence rates and lower OS and DFS rates in the RFA group than in the surgical resection group, respectively. These trends of higher local recurrence and lower OS and DFS rates in the RFA group were maintained for technically resectable or even solitary liver metastasis from CRC. Similarly, a meta-analysis of 26 studies regarding microwave, RFA and surgical resection for liver metastasis from CRC showed that the risk of hepatic recurrence was significantly higher with odd ratio (OR) of 3.94 (p < 0.001) in RFA group comparing with surgical resection group [40]. The OS and DFS at 5 years were also favored surgical resection rather than RFA with hazard ratios (HR) of 1.30 (p=0.003) and 1.40 (p < 0.001) [40]. Especially, the risk of local recurrence was significant higher in subgroups of tumor size of 3 cm or less (OR, 7.26; p < 0.001) and solitary HOCRC (OR, 7.13; p < 0.001) for RFA comparing with surgical resection. The 5-year OS of solitary HOCRC subgroup was significantly superior in surgical resection group comparing with RFA (HR, 1.77; p=0.008) [40]. Therefore, RFA is not sufficient to be compatible with surgical resection as a standard treatment for HOCRC. Various reasons have been proposed to explain the inferiority of RFA. One suggested that resection might remove the occult hepatic micrometastases, which could not be adequately ablated by RFA [39]. Another suggestion was the potential selection bias in the studies in which the patients receiving RFA could have had poorer biological characteristics related to ineligibility for surgery [41].
Despite the inferior outcomes, RFA still remains a valuable option for the HOCRC patients who are ineligible for surgical resection. In addition, neither conclusive results nor established criteria for the modality choice have made through any randomized controlled trial so far. There are ongoing randomized trials comparing RFA with surgical resection including COLLISION trial (NCT03088150), HEL-ARC trial (NCT02886104), and LAVA trial (ISRCTN52040363). COLLISION trial is enrolling the CRC patients with 1–10 liver metastases (size ≤ 3 cm) and no extrahepatic metastasis eligible to both surgical resection and thermal ablation in the Netherlands [51]. HELARC trial, which is being conducted in China, aims to compare the surgical resection and thermal ablation in the CRC patients with 1–3 liver metastases (size ≤ 3 cm) and no extrahepatic metastasis who are suitable to both modalities [52]. In LAVA trial, which is conducted in the United Kingdom and the Netherlands, enrolls high-risk CRC patients with liver metastases who have poor prognostic factors (e.g., poor response after chemotherapy, curable extrahepatic disease, or multiple synchronous metastasis, etc.), and the requirement of high-risk surgery such as staged hepatectomy with or without portal vein ligation or embolization [53]. These trials are expected to provide informative results and to aid in establishing the useful criteria for modality choice.
SABR for Hepatic Oligometastasis
SABR is a widely used RT modality for local ablation of both primary and metastatic tumors leading to the LC rates over 90%. Recently, use of SABR for treatment of OM from various malignancies is expected to increase, based on validation through the SABR-COMET trial, which showed the superiority of SABR compared with standard of care [8]. SABR has also consistently shown excellent LC rates for HOCRC (Table 3), however, there are limited number of studies that evaluated the efficacy of SABR exclusively for the HOCRC patients.
The characteristics of the study population were diverse, including tumor factors, and thus, the reported outcomes were quite heterogeneous. A few certain factors in the patients’ characteristics or treatment parameters, however, consistently showed a significant association with the oncological outcomes in the previous reports. The tumor size was an important independent factor associated with the oncological outcomes. Doi et al. [59] showed tumor size ≥ 30 mm was a significant independent risk factor for low LC rate with HR of 3.940 (p=0.0314). McPartlin et al. [57] reported the sum of gross tumor volume and the presence of extrahepatic disease at the time of SABR as the independent factors for OS (HR, 1.27; p=0.017 and HR, 2.11; p=0.005, respectively). In addition to the tumor factors, the prescribed dose was a critical factor for LC. Joo et al. [58] reported that the 2-year LC rates significantly differed based on the prescribed biologically effective dose (with α/β ratio of 10) of ≤ 80 Gy, 100–112 Gy, and ≥ 132 Gy (52%, 83%, and 89%, respectively). In another study, increasing the minimum dose relative to the gross tumor volume was associated with the improved LC rate of 41% at 4 years in the patients receiving dose ≥ 37.6 Gy when compared with 0% for the others [57]. These results indicated that the candidates with small-sized liver metastasis, low burden of total liver metastasis, absence or control of extrahepatic disease, and higher radiation dose should serve as the selection criteria for SABR to achieve satisfactory LC rates.
SABR has often been compared with RFA for hepatic malignancy, especially, hepatocellular carcinoma (HCC) [41–43]. Because both modalities are non-surgical approaches, the indications of each modality overlap but not the same. Therefore, the choice between these modalities should not be randomly made [60]. RFA is not applicable to the tumors located in the invisible area by ultrasonography, such as the subphrenic area or an area where the probe cannot be properly approached [61]. RFA is also unsuitable for the tumors proximal to the vasculature due to the potential heat sink effect that can reduce the ablation volume and mitigate the LC rate [62]. Furthermore, despite the low complications rates, RFA has the potential to cause procedure-related issues including hepatic bleeding, pleural effusion, biliary fistula, skin burn, pneumothorax, peritoneal seeding, and pleural hemorrhage. Thus, the patients at risk of these complications are not the appropriate candidates of RFA [63,64]. Conversely, the anatomical limitations appear to be less significant issue and seldom relevant in SABR when compared with RFA [65]. Hepatotoxicity and bowel damage adjacent to the target volume, however, are the concerns with the liver-directed SABR [65]. The risk of hepatotoxicity following SABR is associated with radiation dose, irradiated volume, and underlying liver function. The risk of bowel damage depends on the proximity of the target volume to the corresponding bowel. Although the rates of relevant toxicities were reported as < 1% following SABR, proper patient selection considering patient- or tumor-related factors is highly required [63].
No randomized controlled trial that compared both modalities for local ablation of any hepatic malignancy has been reported yet. Though a phase III randomized trial of SABR vs. RFA for HOCRC with one-to-four inoperable hepatic metastases (RAS01, NCT01233544) was initiated by a Danish group, it was terminated early due to the insufficient patients’ recruitment [66]. Currently, there is no ongoing clinical trial of the relevant issue [60]. There are several retrospective studies that compared two modalities [50–55], which generally showed similar LC rates (Table 4). Furthermore, in subgroup analysis, LC rates following SABR for primary HCC or hepatic metastasis > 2 cm tended to be better when compared with RFA. In various studies, as the tumor size increased, the difference in the LC rates was greater following RFA when compared with SBRT. Yu et al. [67] compared RFA and SABR for treatment of HOCRC. They performed subgroup analysis by adjustment with the inverse probability of treatment weighting and showed that SABR resulted in significantly higher LC rate (HR, 0.153; p < 0.001) in the patients’ subgroup with tumor size > 2 cm, while not in the subgroup of tumor size ≤ 2 cm (HR, 0.648; p=0.10), respectively [67]. Similarly, Franzese et al. [68] showed significantly higher LC rate following SABR (91%) when compared with ablative therapy using MWA (84%) in the subgroup of liver metastasis from CRC (p=0.0214), and in the subgroup with tumor size ≥ 3 cm, the discrimination between the modalities were much larger (p=0.005) than in the subgroup with tumor size < 3 cm (p=0.238), indicating that SABR was a better modality for tumor size > 2 cm when compared to RFA. Considering the risk of complications in the gastrointestinal tract, however, RFA can be a better modality for the tumors close to the bowel. For adequate choice of modality, a multidisciplinary approach with consideration of the patient preference is essential.
Future Perspective of RT
As the irradiation technology improved, the use of SABR for liver tumors has increased. Among the advances, introduction of proton beam therapy (PBT) has led to the extended utilization of RT in liver tumors. Compared with X-ray RT, PBT has the Bragg peak phenomenon with a sharp rise and steep drop in the energy deposition along the beam path. The Bragg peak can be expanded to generate a wide range of dosimetric coverage. Due to this peculiar physical property, PBT does not lead to the exit dose that can potentially affect the normal tissue around the target volume. Because liver damage can occur even with low-dose irradiation, RILD is a main concern especially in the patients with poor liver function despite the advances in modern RT technologies. PBT, however, can reduce the irradiated volume in the normal liver parenchyma. Many studies showing the benefit of PBT in liver-directed RT were conducted in treating the HCC patients. Compared with X-ray therapy, PBT enables an increase in the prescribed dose while reducing the risk of RILD [73]. Based on this benefit of PBT, high-dose irradiation has been attempted in PBT for the HCC patients, and the 3-year LC rates of approximately ≥ 80%–85% were reported in various studies. Recently, the first phase III randomized controlled trial in which the clinical outcomes following PBT and RFA were compared among the patients with one or two recurrent HCC < 3 cm was carried out by investigators at the Korean National Cancer Center [74]. Crossover between modalities was allowed if the assigned method was not technically feasible. They reported significantly higher 2-year local progression-free survival in the PBT group on both the per-protocol population (p < 0.001) and intent-to-treat population (p < 0.001), respectively, which satisfied the non-inferiority criterion of PBT to RFA. Furthermore, the rates of crossover to the other arm were significantly higher in the RFA arm (26.4%) than in the PBT arm (8.3%), indicating that PBT was an oncologically equivalent option that could serve as an alternative for the HCC patients who were ineligible for RFA. Although the accumulating clinical evidence shows the benefit of PBT for primary HCC, relevant studies for HOCRC are still very limited. Hong et al. [75] conducted a phase II study of proton-based SABR for liver metastases from various primary tumors including CRC, pancreatic cancer, esophagogastric cancer, breast cancer, and HCC, in which the proportion of CRC patients was 38.2%. The prescribed dose was 30–50 Gy in five fractions, and the 1- and 3-year LC rates were 71.9% and 61.2%, respectively. In the CRC subgroup, the LC rates were significantly lower when compared with the total study cohort (p=0.05). Another phase II study (NCT04456621) of hypofractionated PBT for liver metastasis from various primary malignancies, with CRC of 61.2%, was performed by Kim et al. [76] and the result was published recently. The prescribed doses were mainly 60 Gy in five fractions or 70 Gy in 10 fractions. Actuarial rate of LC at 36 months was more than 60% and none of the patient developed toxicity of grade 3 or more. However, those studies dealt with liver metastasis from diverse primary cancers. There is only one currently ongoing investigation of liver-directed PBT exclusively for HOCRC (NCT03577665) [77]. The study is single-arm phase II study of curative PBT with 72 Gy in 15 fractions for patients with liver metastasis from CRC and the recruitment is ongoing. Although the data are currently limited and more results are necessary, the use of PBT in metastasis-directed therapy for HOCRC may be promising as indicated from the studies on the primary HCC patients.
Establishment of biomarkers for prognosis prediction and selection of candidates for SABR should also be investigated. mCRC has been considered radioresistant in various studies showing worse LC rate after SABR comparing with other primary malignancies [78–80]. The radioresistance of mCRC is explained by the mechanism of molecular effectors in CRC cells [81]. The expression of phosphatase of regenerating liver-3 (PRL-3) gene and survivin, the members of the inhibitor of apoptosis protein family, are specifically upregulated in mCRC comparing with other radiosensitive histologies leading the radioresistance of mCRC [81,82]. Another research by Scott et al. [83] also showed relatively low radiosensitivity of CRC by low genomic-adjusted radiation dose (GARD) of CRC among the diseases of 45 Gy level. Because GARD was derived by radiation sensitivity indices (RSIs) which were calculated based on the expression of 10 genes related with DNA-damage repair, cell cycle, or apoptosis, etc., relatively low GARD of CRC represented relatively high RSI comparing with other primary cancer cells [83]. However, the distribution of RSIs within the CRC subgroup was diverse and further analyses comparing RSIs among the CRC subgroup have not been performed [80]. Besides the differences in genetic expressions, tumor mutations including KRAS, TP53, and HER2 have attracted attention due to their possible association with curability and LC of OM patients [60]. Among the mutations, Hong et al. [75] identified the KRAS mutation as the strongest predictor of inferior LC after PBT-based SABR for liver metastasis from CRC (p=0.02). Furthermore, patients with both KRAS and TP53 mutations showed the worst 1-year LC rate compared with all other genotypes (p=0.001). For more precise selection of modality between RFA and SABR in patients with HOCRC, biomarkers for radiation sensitivity or LC rate after SABR are necessary.
Synergistic effect of RT with systemic therapy would be also an important issue. Recently, the use of immunotherapy has been extended in CRC patients especially with microsatellite instability (MSI) or mismatch repair enzymes deficiency (dMMR) as pembrolizumab showed improved progression-free survival comparing with chemotherapy in MSI-high or dMMR mCRC by KEYNOTE-177 study [84,85]. RT also induced immune modulation, in turn, sometimes resulting in the shrinkage of tumor outside the RT target, so called abscopal effect [86]. Furthermore, the immunologic effect of RT also can potentially augment the effect of immunotherapy [86]. The synergistic effect of RT and immunotherapy has been reported in various cancers [87,88]. For CRC, cases of abscopal effect after carbon-ion RT have been reported [89]. Regarding the combination of RT and immunotherapy, there were some reports support the use of RT can boost the effect of immunotherapy [90]. Especially, RT can potentially enhance the immunotherapy response in microsatellite stable CRC which is considered immunotherapy-resistant [91]. Therefore, for the patient with HOCRC who is considered as a candidate of immunotherapy, RT may potentially improve the progression-free survival by not only enhancing the response of target lesion but also suppressing elsewhere progression. However, there is no relevant study investigating the synergistic effect of immunotherapy and RT for oligometastatic CRC. Therefore, study for this issue would be meaningful.
Conclusion
Classically, the life expectancy of patients with metastatic cancer was expected on a monthly basis, and only palliative systemic treatment was deemed effective. The favorable outcome of surgical resection for CRC patients with liver metastasis shows the possibility that active metastasis-directed treatment could achieve long-term survival. However, although nearly one-third of patients could have long-term survival after surgery, the rest must experience a metastatic cascade again. Therefore, the role of non-invasive approaches such as RFA and SABR, which impose a less burden on patients, has steadily increased.
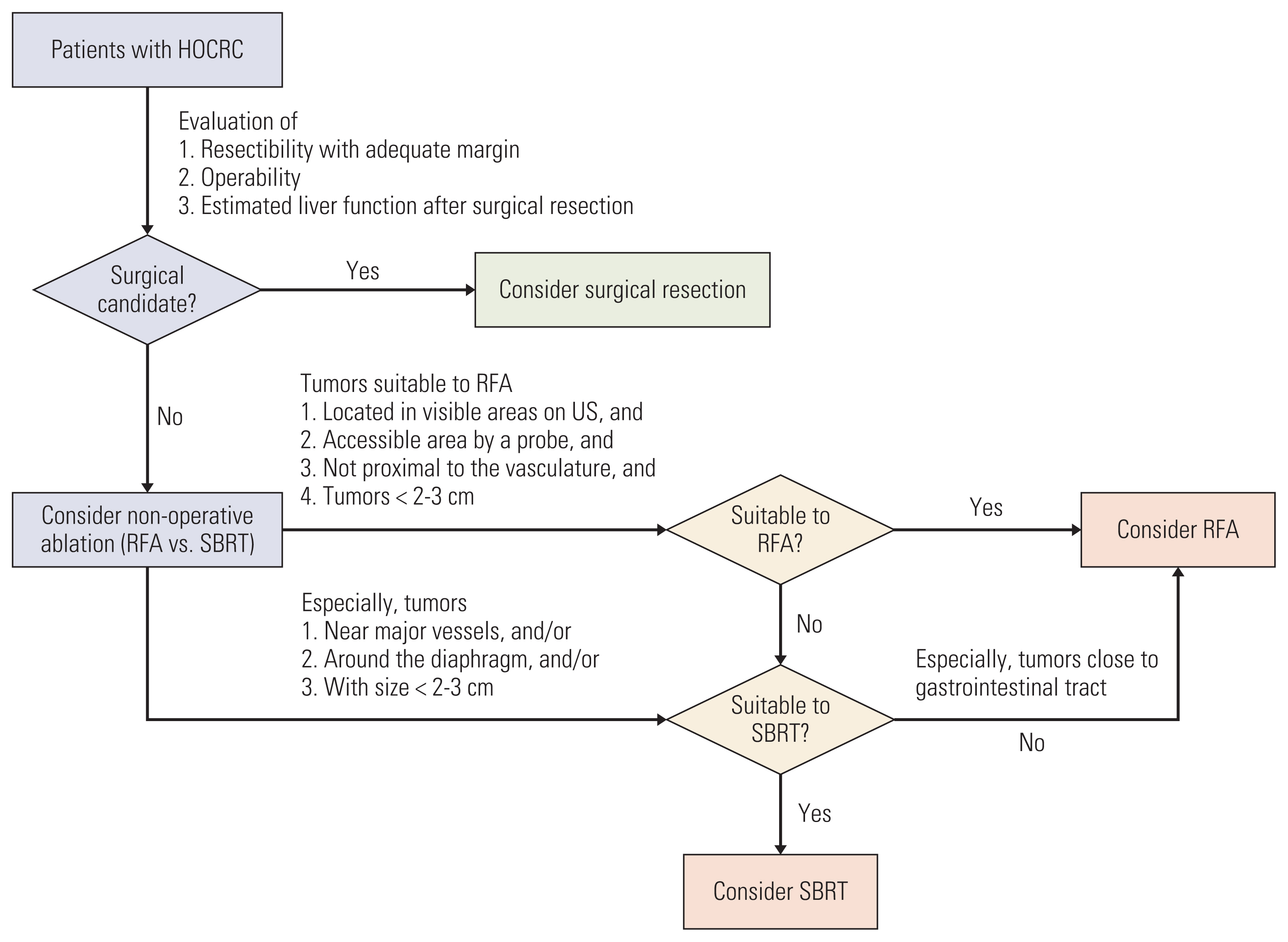
RFA has been an effective tool for treating metastatic liver cancer, however, the LC rates are inferior to those for surgical resection. RFA is also not applicable to tumors located in invisible areas on ultrasonography, in an inadequate area for approach using a probe, or in an area proximal to the vasculature due to the potential heat sink effect. With advances in RT, safe liver-directed irradiation with high-dose is available, and SABR for liver tumor is widely used as complementary tool to RFA. SABR not only provides an LC similar to RFA, but also can safely treat tumors in locations that are difficult to treat with RFA, such as tumors located near major vessels, around the diaphragm, and with large size (> 2–3 cm). The introduction of particle therapy will further reduce the possible toxicities of ablative RT and maximize the efficiency by optimizing the treatment dose. The suggested decision flow is summarized in Fig. 1.
Recent clinical studies of hepatic oligometastasis from CRC investigate the combined effect with systemic treatment as well as the effectiveness of local modality. The distinctive molecular profile of oligometastasis is actively studied, that the results will enable tailored treatments for patients with metastatic disease. SABR or particle therapy is a potent non-invasive modality which can be used in conjunction with novel systemic agents to enhance the therapeutic course of CRC liver metastasis.