Introduction
More than 90% of all thyroid carcinoma are differentiated thyroid cancer (DTC) [1]. Papillary thyroid carcinoma (PTC), a lymphotropic tumor that tends to metastasize to cervical lymph nodes, is the most common type of DTC. Among these lymph nodes, the central neck compartment has the highest risk of metastasis [2]. Although detection techniques such as high-resolution ultrasonography (US) and US-guided fine-needle aspiration (FNA) biopsy greatly improve diagnosis of PTC [3], the sensitivity of US in assessing deep anatomical spaces of the central neck compartment is low [4]. Thus, a considerable number of PTC patients were found to have level VI metastatic lymph nodes when already under surgery or histopathological examinations [5]. In our research, the rate of central lymph node (level VI) metastasis (CNM) whose preoperative examinations showed no lymph nodes metastasis was as high as 36.1% (601/1,663).
Thyroidectomy with central compartment lymph node dissection (CLND) is recommended for PTC patients with CNM. Yet, due to poor reliability of preoperative examinations, prophylactic CLND is not routinely recommended in clinical or radiological node-negative PTC patients, as per American Thyroid Association guidelines. Thus, a tool that helps to quantify the risk of nodal metastasis may facilitate preoperative decision-making [6].
With this objective in mind, our retrospective analysis from two centers was designed using nomogram as the evaluation system, for it excels in user-friendliness and convenience in formulating personalized treatments for a variety of cancers [7,8]. In this study, we covered several factors that could help predict CNM in PTC patients that were absent in the other studies, such as body mass index (BMI), carcinoembryonic antigen (CEA), and creatinine (Cr). Our comprehensive nomogram may aid clinicians in selecting the most appropriate operative strategies to achieve optimal outcome.
Materials and Methods
1. Patient recruitment
Patients who underwent the first-time thyroidectomy to treat thyroid carcinoma at Department of General Surgery, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine (Shanghai, China), and Department of Otorhinolaryngology, Head and Neck Surgery, at the Eye, Ear, Nose, and Throat (EENT) Hospital of Fudan University (Shanghai, China) from June 2016 to June 2019 were studied. A total of 1,731 patients were enrolled (1,294 patients from Ruijin Hospital and 437 from EENT Hospital). The exclusion criteria were as follows: (1) no histologically proven PTC (n=81), (2) no lymph nodes removed (n=68) and had inadequate preoperative blood test report (n=95), (3) pathologically confirmed skip metastasis (n=43), and (4) history or coexistence of other head and neck cancer (n=6). After exclusion, 1,438 patients that had pathological PTC, and received thyroidectomy along with CLND were studied. Among the 1,438 recruits, 1,252 patients (December 2016-May 2019) from both clinical centers were used to make the original model, while 186 patients (June 2019-October 2019) from Ruijin Hospital only were used for external validation.
2. Preoperative examination, surgical strategy, and pathological examination
Preoperative examination including serum index, FNA, and US were performed at Shanghai Ruijin Hospital or Shanghai EENT Hospital. Preoperative US included the following features: type of the surrounding thyroid tissues (normal, Hashimoto thyroiditis, or nodular goiter), tumor size (longest length of the largest lesion), multifocality (more than one nodule scoring higher than Thyroid Imaging Reporting and Data System (TI-RADS) 4A in unilateral thyroid lobe), thyroid capsular invasion (TCI) and suspicious lymph node detected (central lymph node or lateral lymph node).
According to 2010 TNM staging system of the American Joint Committee on Cancer (AJCC) [9], all patients enrolled were identified as T0-4N0-1M0. These patients also received total thyroidectomy or thyroid lobectomy with therapeutic or prophylactic CLND.
All acquired specimens were examined by two or more board-certified pathologists from Shanghai Ruijin Hospital and Shanghai EENT Hospital. Pathological features analyzed were pathological type of tumor, type of the surrounding thyroid tissues, tumor size, multifocality (more than one lesion in unilateral thyroid lobe), and lymph node metastasis.
3. Statistical analysis
We used logistic univariate and multivariate regression analyses to screen risk factors that were significantly associated with CNM using the SPSS ver. 24.0 package (IBM Corp., Armonk, NY). Variables of which the p-value < 0.05 from the univariate logistic regression were then used for multivariate logistic regression to construct a risk prediction model – Nomogram, in R software (ver. 3.5.1, R Development Core Team). The method of decision curve analysis (DCA) was used to evaluate the nomogram model and the US model for prediction of CNM. The decision analytic technique is available in the R statistical package and a step-by-step tutorial is available online [10]. All statistical tests were performed using the R statistical package. The discrimination and consensus degree of our newly-established predictive model were tested through the receiver operating characteristic (ROC) curve, the calibration curve, and the area under the ROC curve (AUC) which is also known as the concordance index (C-index). The likelihood of CNM were quantified as risk scores according to our nomogram, and each patient was stratified into different subgroups by their calculated CNM risk scores.
4. Ethical statement
Consent has been obtained from each patient or subject after full explanation of the purpose and nature of all procedures used. All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Ethics Committee of the Eye and ENT Hospital of Fudan University and the Ruijin Hospital of Shanghai Jiao Tong University School of Medicine, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Results
1. Demographics and clinical characteristics in original model
A total of 1,252 PTC patients including 447 males (35.7%) and 805 females (64.3%) underwent thyroidectomy with CLND in our institution. Mean age was 43.1 years with a range of 14-78 years, and mean BMI was 23.81 with a range of 16.67-43.56. Two serum indexes were included, CEA medium was 1.42 while the Cr medium was 64. Through preoperative US detection, the mean size of tumor size was 0.86 cm with a range of 0.05-6.5 cm. Four hundred ninety-five (39.5%) were diagnosed with thyroid capsule invasion, 373 patients (29.8%) were found to have more than one lesion higher than TI-RADS 4A in the same lobe (multifocality). Among the surgical specimens, 243 (19.4%) were confirmed to have bilateral PTC, 618 (49.4%) were ultimately confirmed to have CNM. The mean harvested central lymph nodes was 7.1, mean positive nodes was 4.3, and 158 patients (12.6%) were pathologically confirmed to have lateral lymph node metastasis (LLNM) (Table 1).
2. Univariate and multivariate analysis of CNM variables
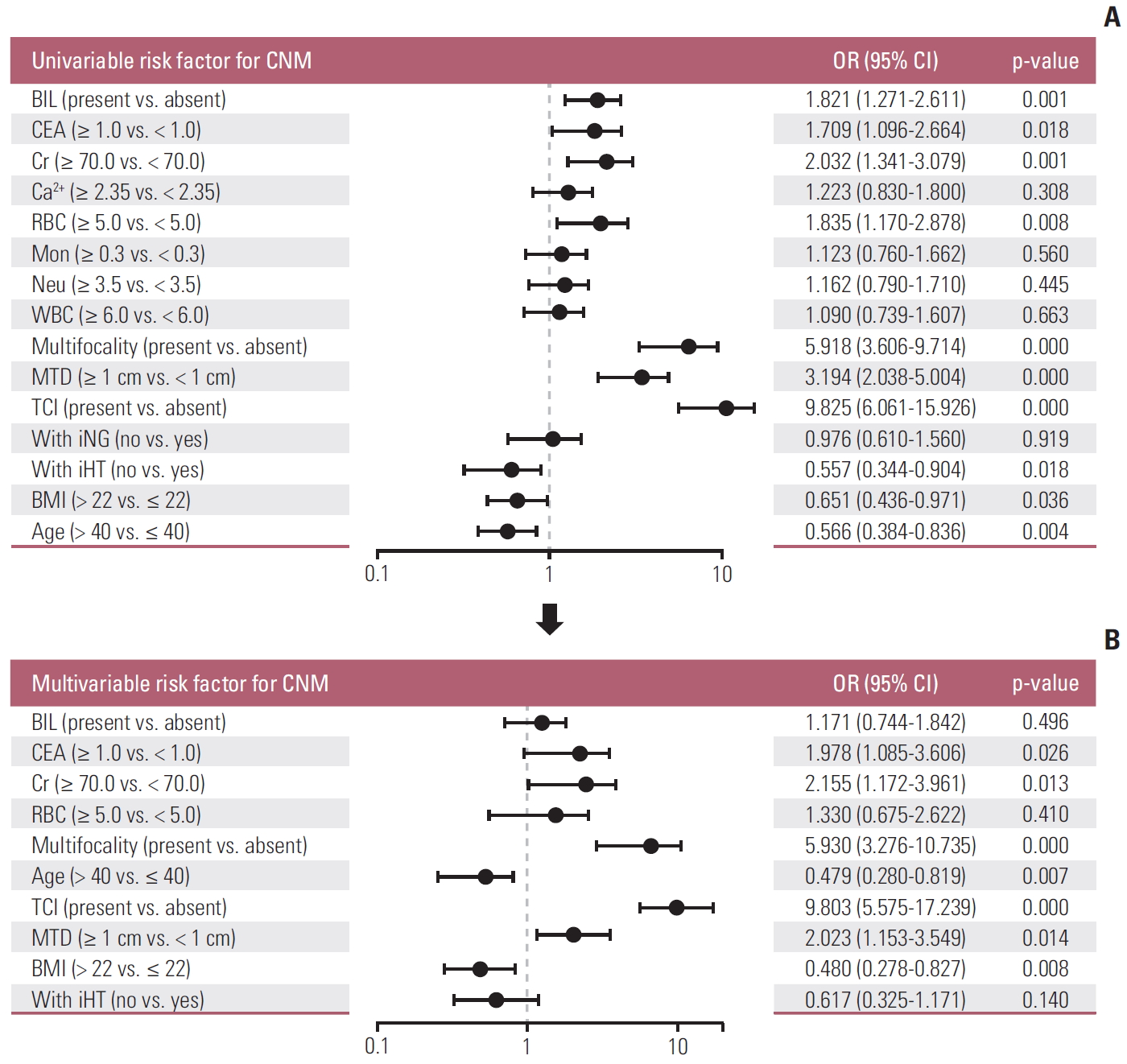
In the univariate analysis, bilaterality (p < 0.001), CEA (p=0.018), Cr (p < 0.001), red blood cell (p=0.008), multifocality (US) (p < 0.001), maximum tumor diameter (MTD, US) (p < 0.001), TCI (US) (p < 0.001), ipsilateral Hashimoto thyroiditis (p=0.018), BMI (p=0.018), and age (p=0.004) have association with CNM (Fig. 1A). Multivariate logistic regression modeling was further conducted to screen for significant variables associated with CNM. Results were as follows: CEA > 1 ng/mL, Cr > 70 μmol/L, multifocality, age < 40 years, TCI, MTD > 1 cm, BMI < 22 (Fig. 1B).
3. Nomogram for predicting likelihood of CNM in PTC patients
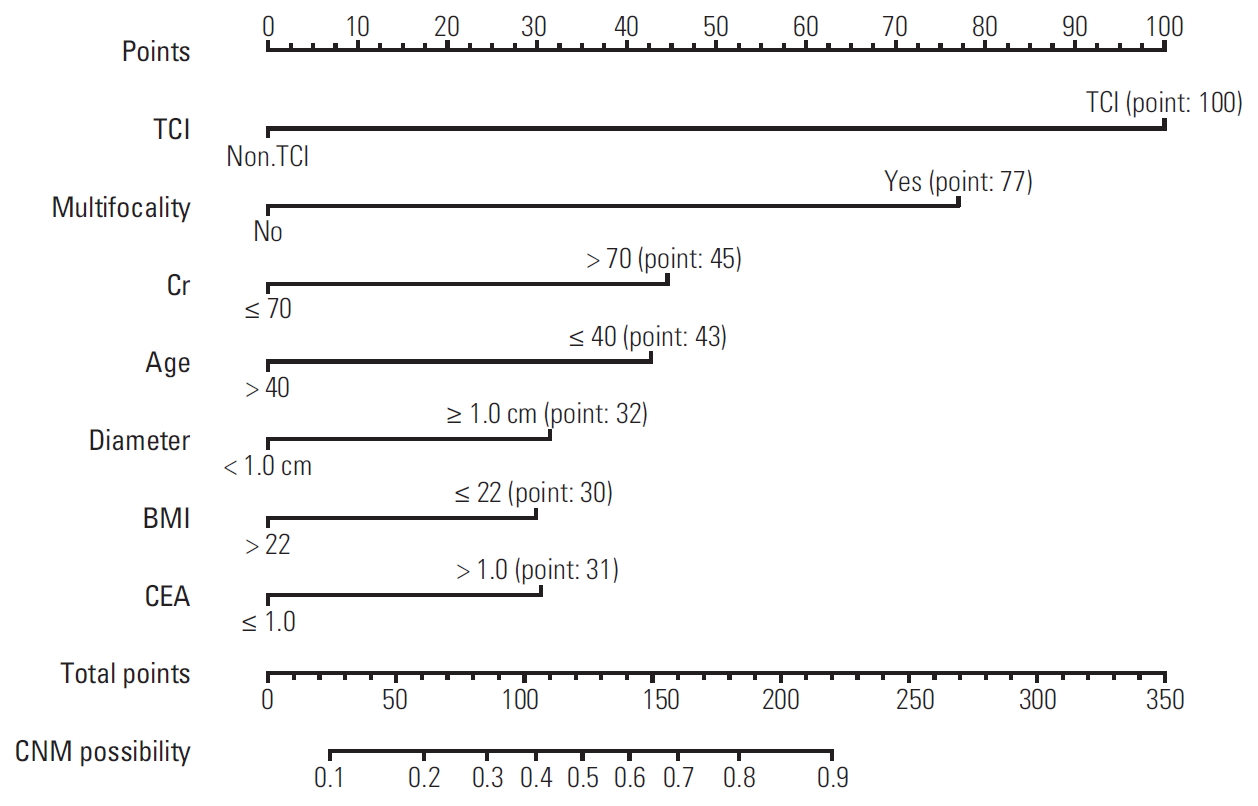
Based on the independent factors screened through multivariate analysis, a nomogram was established for predicting individual risk of CNM. The risk of each factor including CEA, Cr, multifocality, age, TCI, and BMI was quantified in our predicting model (score of each factor was shown in Fig. 2) to predict the presence of CNM in PTC patients.
4. Internal and external validation of the nomogram
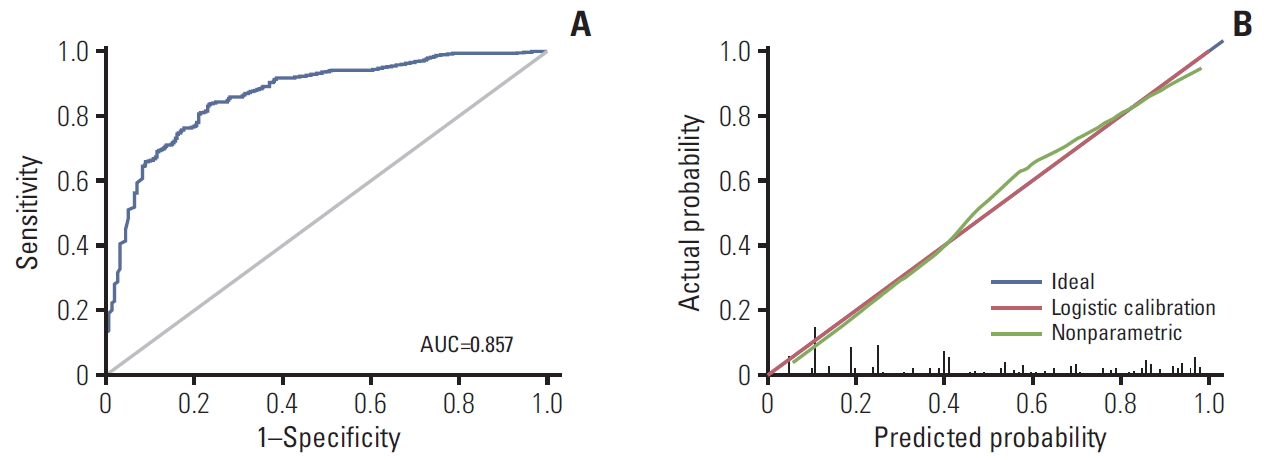
To evaluate our nomogram’s ability to predict CNM in PTC patients, we conducted an internal validation using 1,000 bootstrap resamples. A C-index of 0.857 (95% CI, 0.821 to 0.894) was achieved, and a similar C-index 0.854 (95% CI, 0.843 to 0.867) was acquired after 1,000 bootstrapping, confirming its satisfactory accuracy in predicting central lymph nodes involvement. ROC curve and AUC are presented in Fig. 3A. Furthermore, we also conducted a calibration plot for our newly-established model, and a favorable agreement was shown between the actual and estimated probability of CNM (Fig. 3B). The external validation population comprised of 186 patients (122 females) with a 53% overall rate of nodal metastases. The mean age was 41.8 years with a range of 19-72 years. When applied to the original model, the external validation data set produced a C-index of 0.825 (95% CI, 0.793 to 0.857) (Fig. 4).
5. Validation of the predictive effect of serum factors
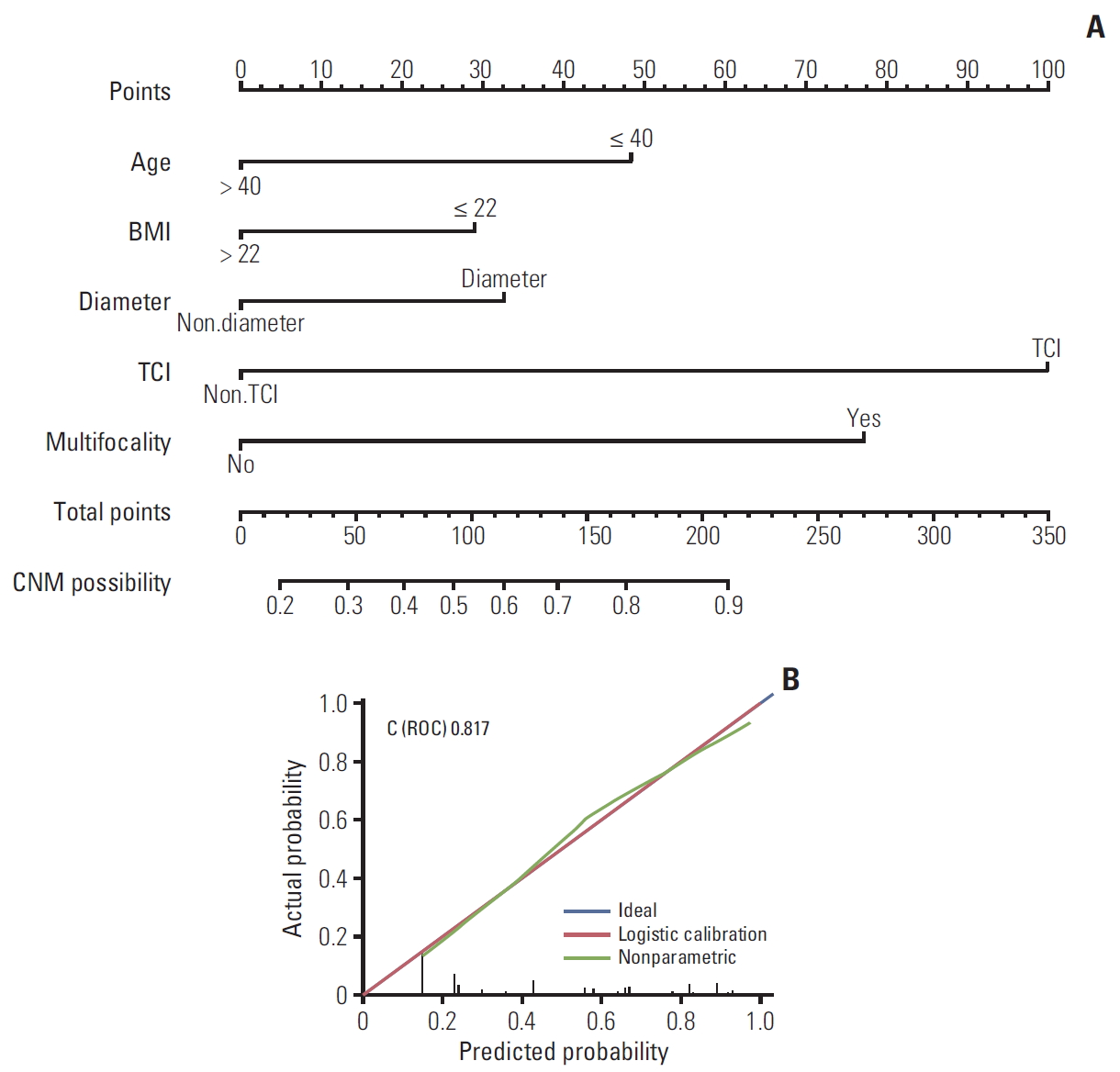
In order to evaluate the effect of serum indicators (CEA and Cr) we included in this prediction model, we excluded two serum indicators and reproduced a contrast nomogram (Fig. 5A), with a C-index of 0.817 (Fig. 5B), proving that these two factors we included were significant and could improve our nomogram’s ability to predict CNM.
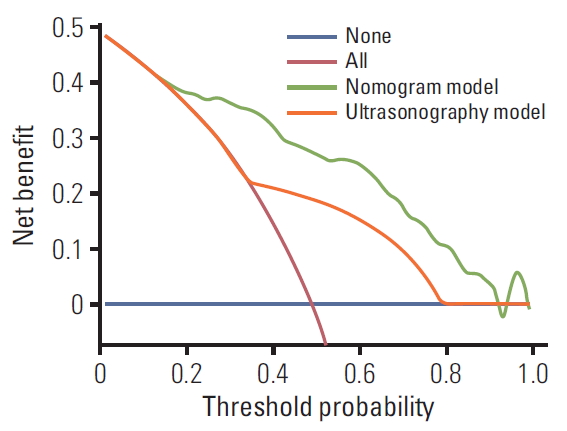
6. Comparing two models in predicting CNM based upon a decision curve analysis
A DCA was performed to compare the predictive ability between our nomogram and the US model. The US model used the data from the preoperative ultrasonographic diagnosis of CNM in our patient cohort (n=1,252). The DCA showed that the prediction ability of our nomogram is superior to US in detecting CNM for PTC patients (Fig. 6).
7. Novel risk stratification according to the scores obtained by the nomogram
Every variable included in our nomogram had its corresponding risk point and total risk scores calculated for all patients to quantitatively predict their individual risk of CNM. To stratify patients according to their risk scores, four cut-off values were selected. Five subgroups were thus established: (1) extreme low-risk group (patients with a CNM score of ≤ 50, n=137), (2) low-risk group (50 < risk score ≤ 100, n=311), (3) moderate-risk group (100 < risk score ≤ 150, n=305), (4) high-risk group (150 < risk score ≤ 200, n=184), and (5) extreme high-risk group (patients with a CNM score of > 200, n=315).
The rates of CNM for extreme low, low, moderate, high, extreme high-risk groups were 8.8%, 17.7%, 41.3%, 77.2%, and 89.8%, respectively. Differences were significant between these subgroups (p < 0.001) (Table 2).
Discussion
Increasing incidence of thyroid cancer has been reported over recent years, and surgical resection is generally accepted to be the most effective treatment for PTC [11], yet the role of prophylactic CLND in PTC continues to be debated. Advocates point that prophylactic CLND in cN0 patient reduces local recurrence which contributes to less hazardous reoperative surgery [6,12,13]. In our country, given the combination of higher CNM risks in Asian patients and unreliability of preoperative examinations in detecting CNM [14], most institutions prefer thyroidectomy with prophylactic CLND. In this study, the rate of patients who received prophylactic CLND was 96.1% (1,663/1,731).
Although there is increasing support for prophylactic CLND given its benefits for recurrence and survival, many clinicians worldwide still opt for therapeutic CLND only, due to potential risks of prophylactic CLND. These could include permanent hypoparathyroidism, recurrent laryngeal nerve injury, and other postoperative complications [15-17]. Furthermore, in the American Thyroid Association guidelines (2015), “less is more” seemed to be the theme running throughout the consensus, recommending less extensive surgeries, less radioactive iodine and less surveillance testing [9,18]. In addition, the importance of regional lymph nodes for cancer survival is stressed in immunotherapy [19], as preservation of normal lymph nodes in meaningful for follow-up treatments. Thus, accurately assessing risks of CNM may play an important role in surgical options, for it is the deciding factor in whether prophylactic CLND should be performed.
Our study aimed to develop a nomogram to predict the likelihood of CNM in PTC patients. A CNM rate of 49.4% was identified, which is in accordance with figures of 40-58% reported by other similar works [20,21]. Among these patients, 158 patients (25.6%) were observed to have LLNM, while 43 patients (3.4%) had skip metastasis (i.e., had LLNM without CNM) which is similar to the observation made by Thompson et al. [6,22]. Given the low prevalence of skip metastasis, most LLNM will be accompanied by CNM, and a routine CLND will be performed; thus, we question the significance of including LLNM as a risk factor for CNM suggested by Wang et al. [23]. However, their results match our finding where there is a significant association between CNM and LLNM, and we will report this clinical research in our following work.
Referencing similar works on predicting CNM, our research confirms their results and takes it a step further. The nomogram developed by Thompson et al. [6] was based on 914 patients and had good discrimination with a C-index of 0.764, while only four variables were considered. The nomograms established by Wang et al. [23] and Kim et al. [24] enrolled larger patient cohorts, yet their discrimination presented a C-index of 0.711 to 0.721, which was weaker than this study. In addition, the equal split of the variables (age and tumor size) in Kim et al.’s work [24] is also quite puzzling given the nonlinear relationship between the variable and CNM according to Thompson’s article [6], which raised further questions about the representative of their nomogram for the general population.
There were a few references on the association between BMI and CNM [25,26], yet our results were quite different to previous findings. Wu et al. [25] found that increased BMI was associated with lymph node metastasis by analyzing a cohort of 796 PTC patients, while we observed that BMI less than 22 kg/m2 was the risk factor for CNM of PTC patients. This difference may be caused by disparate ways of BMI grouping or and the diagnose distinction of lymph node metastasis. However, we believe our nomogram showed a better predictive accuracy (AUC, 0.854) based on greater amount of samples of 1,252 PTC patients.
In this study, we took TCI diagnosed by preoperative US as variable instead of pathological TCI due to the lack of pathologically uniform standard (whether TCI or extrathyroidal extension [ETE]) in our institutions. This stems from a lack of definite definition for TCI or ETE in thyroid pathology [27]. Preoperative US TCI was identified in 39.5% cases, while other studies repor-ted that pathological TCI was present in around 30%-53% cases [6,28,29]. Interestingly, we observed TCI to be the most sensitive characteristic in our nomogram. Several works have proven the connections between TCI or ETE and CNM [23,24] and Thompson et al. [6] found wider spread ETE had a higher likelihood of lymph node metastasis compared to mere capsular invasion.
Multifocality and large tumor size have frequently been shown to promote CNM of PTC patients [2,6,12,20,23,24]. In our research, we obtained similar findings to previous studies, shown in our nomogram (Fig. 2), in which multifocality and tumor size larger than 1 cm both played an important role.
Preoperative serum index is available in most institutions, yet their association with CNM of PTC patients seems to be overlooked. We gathered all the pre-operation clinical serum index including blood routine examination, serum hepatorenal function, serum electrolyte, serum thyroid function, parathyroid hormone and CEA. Interestingly, we found serum Cr and CEA did contribute to our nomogram, suggesting PTC patients with Cr over 70 μmol/L or CEA over 1 ng/mL might suffer a higher risk of CNM.
Above all, this nomogram made it possible to score the likelihood of CNM in PTC patients before operation, which showed a significant advantage over preoperative US (Fig. 6). By gathering readily available clinical characteristics, we divided PTC patients into five quantified risk stratification in our nomogram (Table 2) so that it is easier to use clinically. Using this risk stratification table, clinicians may be better informed in their assessment of the risk factors.
There are several limitations of this study which we hope to address in our following research. Although we gathered patient cohort from two institutions, our sample was not as large as the two recent researches [23,24]. In addition, only 523 patients’ BRAF mutation reports were available and fewer patients received a postoperative immunohistochemical examinations. Future predictive models may incorporate microRNA and PTC subtypes, as well as immunohistochemical biopsy and genotype of FNA samples, which are not available at present. Furthermore, we were able to incorporate several new variables that are significant for prediction of CNM. This implies that there may be potential variables waiting to be discovered that could make the nomogram more complete.
Using available pre-operative variables, we were able to construct a nomogram that stratify PTC patients into five groups that possess different CNM risk levels. This provides guidance for whether a patient should receive CLND on a case by case basis, and promotes balanced approach between avoiding CLND complications and maximizing survival/lowering recurrence rates.