Introduction
Although women 40 years of age or younger account for approximately 6% to 7% of breast cancer diagnoses each year in Western countries, breast cancer is the leading cause of cancer-related deaths in that population [1-3]. The proportion of Asian patients with breast cancer in that age group is reported to be much higher, at 7.6% to 12% [4,5]. The average age at which women have their first child is also rising in Asian countries. As a result, health care professionals are more often confronted with questions regarding pregnancy after breast cancer treatment, including questions about the optimal timing to attempt conception, the consequences for the prognosis of the mother, and the safety of the child. Many women and their physicians are concerned about the negative prognostic effects of the high estrogen levels associated with pregnancy. However, whether breast cancer survivors should be advised against pregnancy remains to be determined. Nonetheless, 70% of young patients with cancer wish to have children after the completion of treatment [6,7].
The proportion of patients with at least one full-term pregnancy after a breast cancer diagnosis is only 3% for women younger than 45 years of age, and 8% for women younger than 35 years of age [8]. Fears related to the negative impacts of pregnancy on the evolution of breast cancer, reduced fertility derived from gonadotoxic therapy, the long duration of endocrine therapy, and the possibility of adverse obstetric outcomes may explain why those patients have such low pregnancy rates [9].
Although numerous studies have assessed the pregnancy outcomes and the prognostic impacts of pregnancy among patients with breast cancer, those topics have received little attention in Asian countries [10-17]. Studies of pregnancy outcomes subsequent to breast cancer treatment require a large number of young patients with breast cancer and a long follow-up period. We evaluated the incidence and outcomes of pregnancy after breast cancer in women of childbearing age in a large cohort of Korean women.
Materials and Methods
1. Data sources
We used data from the Korea National Health Insurance (KNHI) database, which were linked to cancer registration and mortality data from the Korean National Cancer Registry (KNCR) and the Korea National Statistics Office (KNSO), respectively. The KNCR is a population-based regional cancer registry in the Republic of Korea. In 2005, the KNCR began to release data collected since 1999 that was suitable for research [18]. By 2012, the completion rate for cancer registration in the KNCR reached 97.7% [19]. Since the implementation of the National Health Insurance Act in 1989, almost 97% of the Korean population has been subject to compulsory health insurance provided by the KNHI. The KNHI currently manages the entire health claims database in Korea and provides research data on enrollees, sampled using a proportional allocation method with adherence to a strict confidentiality policy. The KNHI, KNCR, and KNSO databases have been used for epidemiologic studies in the past and are considered to be of high quality [20-24]. We also conjugated this linked database to define our study variables. For example, the variables for cancer type, cancer diagnosis date, and breast cancer incidence were extracted from the KNCR database; the variables for pregnancy status, pregnancy outcomes, treatment of breast cancer, and dates of recurrence were extracted from the KNHI database. The variables for cause and date of death were extracted from the KNSO database. Specific information regarding the databases used in this study are available elsewhere [25].
2. Identification of the study population
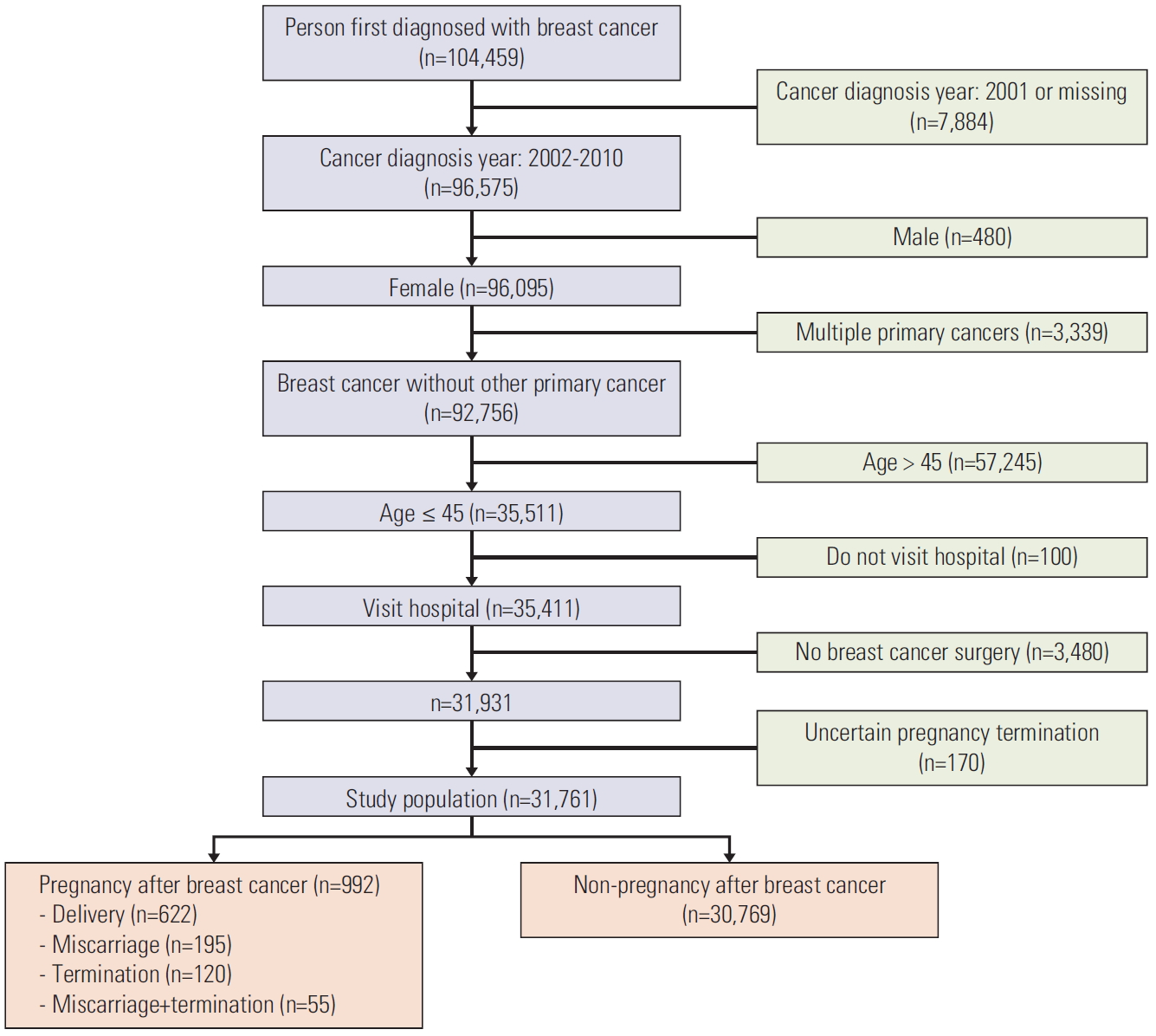
Data for a population of women who received a first-time breast cancer diagnosis (International Classification of Diseases, tenth revision [ICD-10] code C50) were extracted from the KNCR for the period of January 1, 2002 to December 31, 2010. We excluded patients who were male, who had multiple primary cancers, and whose age at diagnosis was > 45 years. Use of the KNHI database allowed us to exclude patients who did not visit the hospital and who did not have breast cancer surgery. Patients with an unknown pregnancy result were also excluded. A total of 31,761 participants were selected for this retrospective, population-based cohort study (Fig. 1).
We grouped the study population into two categories depending on pregnancy status. We identified patients with an ICD-10 code beginning with “O” as pregnant individuals and those without such an ICD-10 code during the follow-up period as non-pregnant individuals. We further divided the pregnant individuals into two groups depending on the pregnancy outcome: successful delivery and failed to deliver. We defined breast cancer recurrence in the study population as conditions requiring a new regimen of chemotherapy or endocrine therapy (e.g., aromatase inhibitor or fulvestrant), ≥ 1 year after the initial breast surgery or adjuvant chemotherapy. Recurrence-free survival was defined as the period from the date of breast cancer diagnosis to the date of recurrence event. Overall survival was defined as the period from the date of breast cancer diagnosis to the date of death from any cause.
3. Statistical analysis
We used chi-square tests and independent t tests to compare categorical and continuous variables, respectively. We also used 1:1 propensity score matching analysis [26] of the study cohort to reduce the effects of bias on the estimation of treatment between pregnant and non-pregnant individuals; this bias had the potential to affect the results for recurrence and survival. For this matching, we used the statistical software package ‘matchit’ of R, and controlled the variables for age at breast cancer diagnosis, adjuvant hormonal therapy, chemotherapy, and radiotherapy for the propensity score matching. We compared the overall recurrence and survival rates between the pregnant and non-pregnant groups using the Kaplan-Meier method. Finally, we used Cox proportional hazards regressions to estimate the hazard ratios (HRs) and 95% confidence intervals (95% CIs) for the relationship between pregnancy and survival. We considered p-values of < 0.05 to be statistically significant. We performed all analyses using SAS ver. 9.4 (SAS Institute Inc., Cary, NC); R was implemented in RStudio ver. 1.1.414 (RStudio Inc., Boston, MA).
Results
1. Clinical characteristics of the study cohort
The study cohort included 31,761 women 45 years of age or younger with primary breast cancer. Among them, 992 women (3.1%) had become pregnant after receiving treatment for breast cancer. The median time from breast cancer diagnosis to pregnancy was 1,153 days. The median age at the time of conception was 35.1 years (range, 23 to 51 years).
The characteristics of the study population are summarized in Table 1. Compared with those who did not become pregnant, the women who became pregnant were younger (mean age, 31.8 years vs. 39.6 years; p < 0.001), and lower frequencies of chemotherapy (32.1% vs. 35.2%, p=0.044), adjuvant hormonal therapy (36.9 vs. 61, p < 0.001), and regional Surveillance, Epidemiology, and End Results (SEER) stage (18.5% vs. 27.4%, p < 0.001), which suggested that their cancer was diagnosed at an earlier stage.
2. Pregnancy patterns of young breast cancer survivors
Among the 992 women who became pregnant, 622 experienced a successful delivery (including 268 nulliparae and 83 primiparae or multiparae), whereas 370 failed to deliver. Those who successfully delivered were younger (mean age, 30.6 years vs. 33.9 years; p < 0.001) and had lower frequencies of chemotherapy (29.4% vs. 36.5%, p=0.021) and adjuvant hormonal therapy (33.9% vs. 41.9%, p=0.012). They were also less likely to have become pregnant < 2 years after the breast cancer surgery (17.7% vs. 34.1%, p < 0.001), compared with those who failed to deliver (Table 2).
The results for the characteristics of the study population after propensity score matching are presented in Table 3. After matching, our results indicated that the women who became pregnant after treatment for breast cancer had no differences in age at diagnosis, chemotherapy, radiotherapy, ovarian preservation, trastuzumab therapy, adjuvant hormonal therapy, or SEER state, compared with those who did not become pregnant.
3. Pregnancy and prognosis of young breast cancer survivors
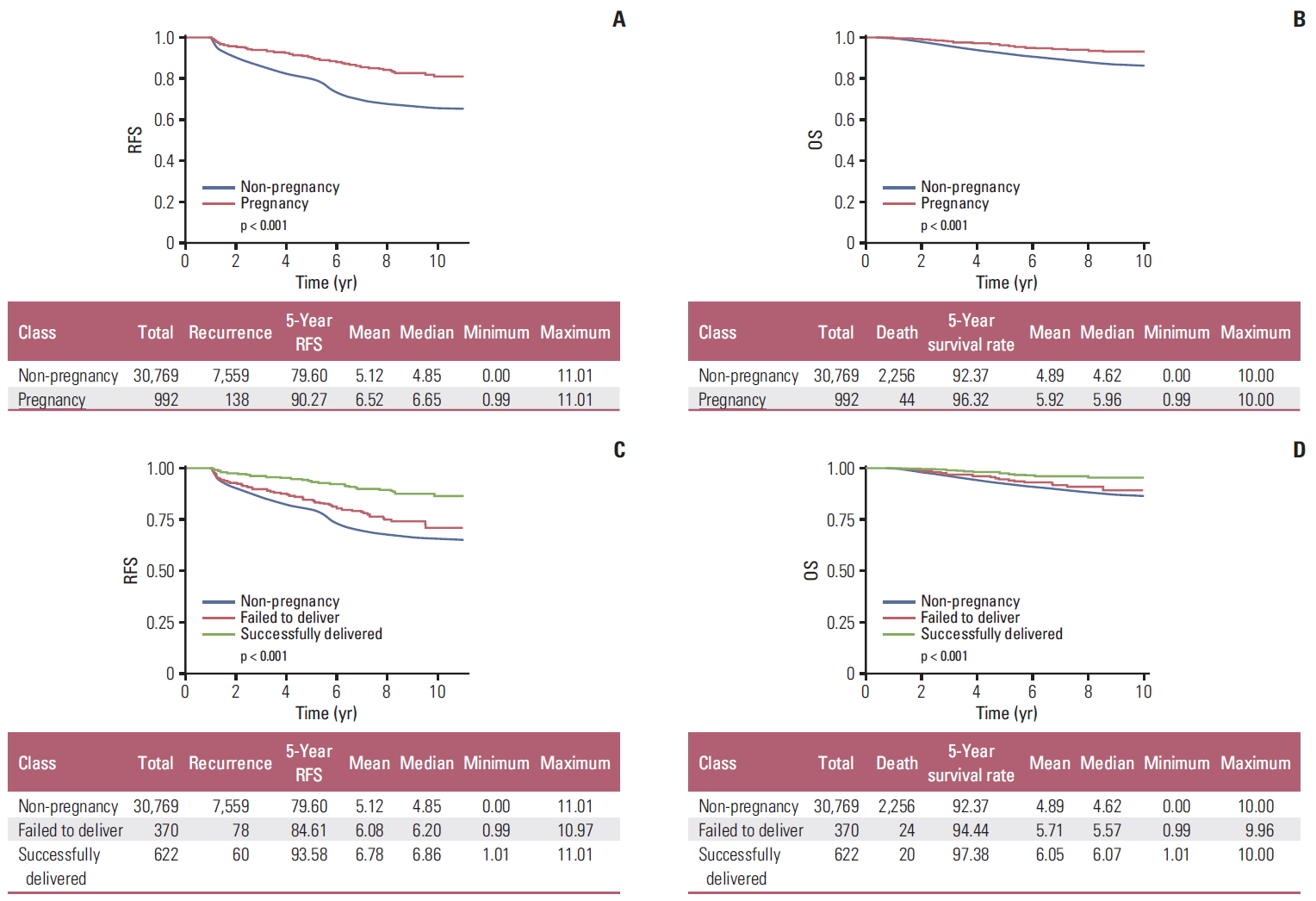
Compared with women who did not become pregnant subsequent to receiving breast cancer treatment, those who became pregnant had significantly reduced risks of recurrence and death. Compared with those who failed to deliver, those who successfully delivered had a lower risk of recurrence and death (Fig. 2, S1 and S2 Tables). After propensity score matching (Table 4, Fig. 3A, C, E and G), our results showed that women who became pregnant had a significantly reduced risk of recurrence (HR, 0.487; 95% CI, 0.398 to 0.595). Furthermore, compared with that for women who did not become pregnant, the risk of recurrence was lower for those who successfully delivered (HR, 0.317; 95% CI, 0.235 to 0.429). However, women who failed to deliver did not have a significantly lower risk of recurrence, compared with that for those who did not become pregnant. (HR, 0.760; 95% CI, 0.561 to 1.030).
After propensity score matching, our results showed that women who became pregnant had a significantly reduced risk of death compared with those who did not become pregnant (HR, 0.487; 95% CI, 0.398 to 0.595) (Table 5, Fig. 3B, D, F and H). Compared with that among women who did not become pregnant, the risk of death was lower among women who successfully delivered (HR, 0.317; 95% CI, 0.235 to 0.429). However, it was not significantly different from that of women who became pregnant but failed to deliver (HR, 0.760; 95% CI, 0.561 to 1.030).
Discussion
We addressed for the first time the outcomes of pregnancy subsequent to a diagnosis of breast cancer among women in Korea. Compared with Western countries, Asian countries have a low incidence of breast cancer and a high proportion of young patients who are able to conceive. Our data showed 38% of women with breast cancer were younger than 45 years old. Studies of the outcomes of pregnancy after breast cancer require large numbers of patients of childbearing age, so there have been very few such studies in Asian countries. To overcome that hurdle, we used data from the KNHI, KNCR, and KNSO databases, which contain high quality data taken from large cohorts and have been used previously for epidemiologic studies [20-24]. Our results showed that 3.1% of young women who were diagnosed with breast cancer became pregnant subsequent to the diagnosis, and furthermore, that pregnancy after breast cancer was not detrimental to the oncologic outcome.
Pregnancy rates are approximately 70% lower among cancer survivors, compared with the general female population [27,28]. In our study, the proportion of women who conceived after receiving breast cancer treatment was lower than the proportion of the general population who conceived. The percentage of women who conceived in our study (3.1%) was similar to a Danish population-based study, which found that 3.6% (371 of 10,295) of women experienced pregnancy [17]. In our study, 622 (62.7%) of the women who became pregnant subsequent to receiving breast cancer treatment delivered successfully. Compared with the women who conceived but did not successfully deliver, those who successfully delivered were younger, waited longer to become pregnant after being treated for cancer, and had a higher frequency of localized SEER stage. Importantly, the outcomes of pregnancy after breast cancer treatment have rarely been investigated in Asian countries. In our study, more than half of the women who became pregnant after receiving breast cancer treatment had a successful delivery.
Concerns about the safety of pregnancy for breast cancer survivors remain high. Health care providers may be uneasy about promoting pregnancy after breast cancer, especially with the current lack of randomized controlled trials, which are ethically difficult to implement. The primary concern regarding pregnancy after breast cancer has been the possible negative impact of pregnancy on the prognosis of patients. Furthermore, the high serum levels of pregnancy-related hormones are known to act as growth factors that affect breast cancer. A large population-based study and a meta-analysis found no difference, however, in recurrence or survival between breast cancer survivors who became pregnant and those who did not become pregnant after breast cancer treatment [8,17,29,30]. Recently, a population-based, retrospective cohort study using health administrative databases in Canada was reported [30]. The study analyzed data from 7,553 women with invasive breast cancer, aged 20 to 45 years at the time of diagnosis. The authors found that the 5-year actuarial survival rate was 96.7% (95% CI, 0.941 to 0.993) for women who became pregnant 6 months or more after their diagnosis of breast cancer, compared with 87.5% (95% CI, 0.865 to 0.884) for women who did not become pregnant (age-adjusted HR, 0.22; 95% CI, 0.10 to 0.49; p < 0.001).
Because of the limitations of the information from the KNHI, KNCR, and KNSO databases, we could not determine the exact cause of the better survival outcome, which was likely linked to earlier SEER stage and better tumor characteristics. Our results indicated that pregnancy after breast cancer treatment was not related to a poor survival outcome, both before and after propensity score matching. This result was consistent with the results of previous studies [8,17,29,30].
Our study used only data from the KNHI, KNCR, and KNSO databases, so there were several limitations. First, we could not investigate information that was not recorded in the databases. Therefore, we could not know the pregnancy outcomes for women who did not visit the hospital after becoming pregnant and as such, the outcomes of 170 pregnancies were unknown. Second, we did not have information about the clinical and pathologic staging, or pathologic parameters, such as estrogen receptor, progesterone receptor, and HER2 status, which is one of the crucial prognostic factors in breast cancer. Therefore, we could not determine how differences in staging, estrogen receptor, progesterone receptor, and HER2 status between women who became pregnant and those who did not become pregnant affected the prognostic results. Third, information regarding parity is known only for women from the KNHI and KNCR databases who had successful deliveries. Fourth, the registration system for the SEER stage has stabilized since 2006 in Korea, and therefore, a substantial proportion of SEER data was missing in our data. Lastly, exact information about cause of death and recurrence were not included in the KNHI and KNCR databases. Therefore, we had to define recurrence using an alternative definition, and information about recurrence in the population could be unclear.
This is the first study to identify the outcomes of pregnancy after breast cancer in Korea using the KNHI, KNCR, and KNSO databases. Our results showed that 3.1% of women of childbearing age who were diagnosed with breast cancer became pregnant after receiving treatment for breast cancer, and more than half of those women experienced a successful pregnancy. As our result of study, breast cancer survivors who became pregnant had a better long term survival compared with those who did not become pregnant. Our results suggest that women can plan to conceive after completing breast cancer treatment without fear of negative effects on recurrence.