Introduction
Gastric cancer is the most common cancer and the third leading cause of cancer death in Korea (1,2). The majority of patients initially present with locally advanced or metastatic disease. Even those patients who are potentially curable have high rates of both local and distant recurrence. Combination chemotherapy was proven to produce a better quality of life and to increase overall survival when compared with the best supportive care for patients with advanced gastric cancer (AGC) (3-5). However, about half of patients do not respond to the current first-line chemotherapy and even the responders eventually show disease progression. After failure of first-line chemotherapy, many of these patients still have a good performance status and adequate organ function, and so they can be candidates for effective salvage treatments. However, a standard salvage treatment has not yet been established.
Oxaliplatin is a third generation platinum compound with the 1,2-diaminocyclohexane (DACH) carrier ligand. Oxaliplatin has shown efficacy against many tumor cell lines, including some that are resistant to cisplatin and carboplatin (6). In addition, it has demonstrated additive or synergistic activity, and especially when combined with 5-fluorouracil (FU) and even for treating 5-FU-resistant cell lines (7,8). A biweekly oxalipaltin plus infusional 5-FU and leucovorin (LV) regimen had a significantly superior outcome for patients with metastatic colorectal cancer as compared to that of 5-FU/LV alone (9). In several phase II studies, FOLFOX-4 showed response rates of 38~43% and a manageable toxicity profile as a first-line treatment for patients with AGC (10,11).
With this background, we conducted a phase II study to determine the effectiveness and safety of FOLFOX-4 when this is used as a salvage regimen for previously treated patients with advanced or metastatic gastric cancer.
Materials and Methods
1. Patient eligibility
All the study patients were required to fulfill the following eligibility criteria: (1) histologically proven gastric adenocarcinoma; (2) tumor progression after prior chemotherapy for metastatic or locally advanced disease; (3) >4 weeks had passed since undergoing prior chemotherapy; (4) no previous exposure to oxaliplatin; (5) measurable lesion that can be accurately measured in at least one dimension (longest diameter ≥1 cm with spiral CT); (6) age more than 18 years; (7) Eastern Cooperative Oncology Group (ECOG) performance status ≤1; (8) adequate bone marrow (absolute neutrophil count ≥1,500/mL, platelet count ≥100,000/mL); (9) adequate hepatic function [bilirubin level ≤1.25 upper limit of normal (ULN), hepatic transaminase ≤2.5 ULN; in the presence of hepatic metastases, bilirubin level ≤1.5 ULN and hepatic transaminase ≤5 ULN]; (10) adequate renal function (serum creatinine <1.5 mg/dL) and (11) estimated life expectancy of at least 3 months. Patients were excluded from study if they had peripheral neuropathy of any grade, central nervous system metastases and an uncontrolled comorbid illness or other malignancy. This study protocol was reviewed and approved by the Gil Medical Center (Incheon, Korea) institutional review board. Written informed consent was obtained from all the patients.
2. Treatment schedule
The patients received oxaliplatin 85 mg/m2 as a 2-hour infusion on day 1, and LV 200 mg/m2 as a 2-hour infusion followed by bolus 5-FU 400 mg/m2 and a 22-hour infusion of 5-FU 600 mg/m2 on days 1 and 2. This treatment was repeated every 2 weeks. Treatment was continued until disease progression or unacceptable toxicity occurred or the patient declined further treatment.
The dose modifications were based on the hematologic parameters and the degree of non-hematologic toxicities. A physical examination, chest x-ray, complete blood counts and biochemical tests were performed before each chemotherapy cycle. The toxicity grading was based on the National Cancer Institute Common Toxicity Criteria (version 3.0). Chemotherapy was delayed until recovery if the neutrophils decreased to <1,500/mm3 or the platelets decreased to <100,000/mm3 or for the patients with significant persisting non-hematologic toxicity. The dose of 5-FU was reduced by 25% when grade 3/4 diarrhea, stomatitis or dermatitis occurred. The oxaliplatin was reduced by 25% for the patients with grade 3/4 neutropenia. For the cases of persistent (14 days or longer) painful paresthesia or functional impairment, the oxaliplatin was omitted from the regimen until recovery.
3. Evaluation
The tumor responses were classified according to the Response Evaluation Criteria in Solid Tumors (RECIST). The response was evaluated based on the findings of a computed tomography (CT) scan with each assessment being done using the same imaging technique as that at baseline. The clinical responses were assessed every 3 courses of chemotherapy or earlier in the case of clinical deterioration.
4. Statistical analysis
The primary end point of the study was the objective response rate. The secondary end points consisted of toxicity, progression-free survival (PFS) and overall survival (OS). Forty evaluable patients were required for a single-stage phase II clinical study with assuming that the expected overall response rate would be 25% and the threshold rate was 10% (alpha and beta-errors set at 0.1).
Survival analysis was performed by the Kaplan-Meier method. PFS was calculated from the date of the beginning of treatment to that of clinical progression. OS was defined as the interval between the date of the beginning of treatment and the date of death or the last follow-up appointment. Cox's proportional hazard method was used for assessing the independent prognostic factors. Statistical significance was calculated at the 95% confidence interval (p<0.05). All the analyses were performed using SPSS for windows 15.0 (SPSS Inc., Chicago, IL).
Results
1. Patients characteristics
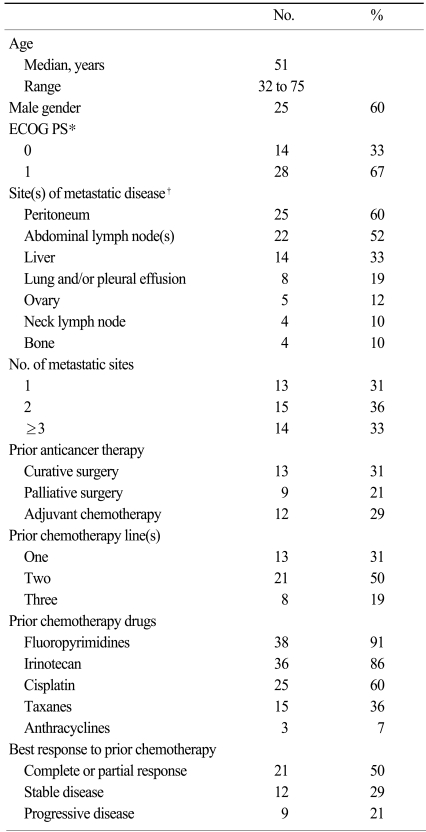
A total of 42 patients were enrolled in the study between August 2004 and March 2007. The patient characteristics are listed in Table 1. The median age was 51 years (range: 32 to 75). Twenty-eight patients (67%) had an ECOG performance status of 1. The main metastatic sites were the peritoneum (60%), the abdominal lymph node(s) (52%) and the liver (33%). Twenty-nine patients (69%) received FOLFOX-4 as more than their third-line treatment. Fluoropyrimidines and irinotecan were commonly used as prior chemotherapy regimens. Twenty-five patients (60%) had previously received cisplatin-based chemotherapy. Twenty-one patients (50%) had achieved a clinical response to their prior chemotherapy.
2. Efficacy
Thirty-eight patients were evaluable for response. The response was not assessable in four patients due to follow-up loss (n=1), the patient's refusal for further treatment after the first cycle (n=1) and death of patients before the completion of the second cycle (n=2). According to the intent-to-treat principle, 9 partial responses were observed, giving an overall response rate of 21% [95% confidence interval (CI), 8 to 34%]. The median duration of the response was 4.6 months. Taking into account the 14 patients who had stable diseases, 23 patients (55%) achieved clinical benefit, which was defined as a partial response or stable disease. There was no significant difference in the response rate between the patients who had previously received platinum-based regimens vs. the patients who had not (29 vs. 16%, respectively, p=0.446). The main reasons for treatment discontinuation were disease progression (67%), patient refusal (14%) and toxicity (12%). After the median follow-up duration of 16.6 months, the median PFS and OS were 3.0 months (95% CI, 2.0 to 4.0 months) and 6.2 months (95% CI, 4.3 to 8.1 months), respectively (Fig. 1).
We conducted univariate analysis of the baseline characteristics such as age, gender, ECOG performance status, the response to previous therapy, the number of previous chemotherapy regimes the patient had undergone, having undergone previous cisplatin-based therapy and the number of organs with metastatic tumor.
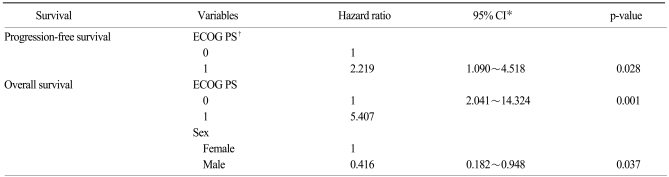
As shown in Table 2, the performance status had a significant impact on both the PFS (p=0.024) and the OS (p=0.001). The PFS and OS for the patients with an ECOG of 0 were 5.1 and 10.8 months, respectively, and the PFS and OS for the patients with an ECOG of 1 were 2.5 and 4.9 months, respectively. Multivariate analysis (Table 3) also showed that the performance status was the only independent prognostic factor affecting both the PFS [hazard ratio (HR), 2.219; 95% CI, 1.090~4.518; p=0.028] and OS [HR, 5.407; 95% CI, 2.041~14.324; p=0.001].
3. Safety
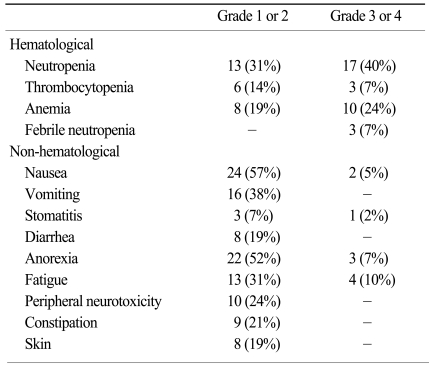
Forty-two patients received a total of 228 cycles of chemotherapy, with a median number of five cycles per patient (range: 1 to 12). The frequencies of the treatment-related hematological and non-hematological toxicities are listed in Table 4. The most common hematological toxicity was grade 3/4 neutropenia, which occurred in 17 patients (40%). Febrile neutropenia was observed in three patients (7%), but this was successfully treated without administering hematopoietic growth factors. Gastrointestinal toxicities were the most common non-hematological toxicities, while severe gastrointestinal toxicities were uncommon: grade 3/4 anorexia, nausea and stomatitis were observed in three (7%), two (5%) and one (2%) patients, respectively. Ten patients (24%) experienced grade 1/2 peripheral neuropathy, but there were no cases of grade 3/4 peripheral neuropathy. One patient died of pneumonia 11 days after the first cycle, and this was considered likely to be treatment-related. Mean relative dose intensities of oxaliplatin and 5-FU were 82% and 83%, respectively. Dose reduction was required in 73 cycles (32%). Treatment was delayed due to toxicities in 52 cycles (23%) of chemotherapy.
Discussion
Chemotherapy has been shown to improve patient survival as compared with best supportive care (BSC) alone for patients with AGC (3-5). However, most patients eventually develop progressive disease. Many patients and physicians request further treatment after failure of the first-line chemotherapy. However, there is no established second-line therapy and the benefit of second-line chemotherapy is not yet clear. A previous study by De Vita et al. (11) suggested that salvage chemotherapy for AGC patients might have a beneficial effect on survival: the patients (n=36) who received a second-line treatment showed a significant better median OS than the patients (n=25) who received only BSC after failing the first-line treatment (12.7 vs. 9.4 months, respectively; p=0.0026). To date, many phase II trials have assessed the activity of second-line chemotherapy on the basis of the radiological response alone. The assessment of symptomatic benefits is also important since chemotherapy for AGC is mainly focused on palliation. Several trials have reported the improvement of disease-related symptoms from second-line therapy (12-16). Furthermore, symptomatic benefits were achieved even in patients who showed no objective response (13,15,16). The first randomized phase III tiral in Germany has recently demonstrated irinotecan as 2nd-line chemotherapy significantly improved OS and tumor-related symptoms compared with BSC (17). Although only a small number of patients (n=40) was evaluated due to poor accrual, second-line chemotherapy can be considered to be a proven option for treating gastric cancer.
This phase II study was designed to assess the activity and safety of the FOLFOX-4 regimen for previously treated patients with AGC. In our study, the response rate (RR) was 21% and the median OS was 6.2 months. These results are comparable with those reported by other phase II trials that have evaluated different FOLFOX regimens (18,19). Kim et al. (18) reported a 26% RR with a median OS of 7.3 months for previously platinum-treated patients. Seo et al. (19) reported a 23% RR with a median OS of 8.0 months with using a modified FOLFOX-6 regimen as salvage therapy. In other phase II trials using some new drugs such as irinotecan and taxanes, the RR has ranged from 14% to 29% with the overall survival ranging from 5.2 to 8.0 months (12,13,20,21).
The most common toxicity in our study was neutropenia. Grade 3/4 neutropenia and febrile neutropenia developed in 40% and 7% of patients, respectively. However, in another phase II study using a different FOLFOX regimen, grade 3/4 neutropenia was observed only 15% of the patients (19). A possible explanation for the relatively frequent incidence of neutropenia is that patients in our study were heavily pretreated. Many patients (69%) received the FOLFOX-4 regimen as a third- or fourth-line treatment. On the other hand, peripheral neuropathy was seen in a minority of patients. The incidence of grade 1/2 neuropathy was 24% without any severe neuropathy. It might be explained by the relatively low cumulative dose of oxaliplatin (median 440 mg/m2, range 85~1,014 mg/m2) our study patients received because chronic neuropathy is cumulative and it is most commonly seen in patients who have received total doses ≥540 mg/m2 (22).
Salvage chemotherapy is not appropriate for all patients. Therefore, the proper selection of patients who are likely to benefit from salvage chemotherapy is important. In our previous study with mitomycin C plus S-1 second-line chemotherapy (23), the patients with a poor performance status (ECOG 2) demonstrated significantly lower survival compared with that of the patients with a good performance status (ECOG 0 or 1). So, we confined the candidates for this phase II study to the patients with an ECOG of 0 or 1. Wilson et al. (24) has suggested that second-line therapy is more likely to be effective in platinum-naive patients. However, in our study, the cisplatin-naive patients did not show a significantly better response and longer survival. The performance status (ECOG 0 vs. 1) was found to be the only independent prognostic factor for both PFS and OS. This might suggest that oxaliplatin has no cross-resistance with cisplatin, and the patients with a good performance status could be good candidates for salvage FOLFOX-4 therapy.