Introduction
Thanks to the global improvement of health care and living conditions, the world population is aging. Already, in developed countries, half of the cancers occur in patients aged 70 and older. In booming Asian nations, such as South Korea, the aging trend is particularly striking, and therefore geriatric oncology is rapidly coming at the foreground of oncology practice. In this article, we plan to review the main acquisitions of this field over the last decades, as well as the areas of present critical research.
Conceptual Frameworks
The notion of geriatric oncology was first articulated in the eighties by pioneers such as Rosemary Yancik, Paul Carbone and Jerry Yates (1). Some of the early studies, mostly retrospective reviews of study data, also started in the eighties (2,3). Over the last twenty years, the framework of the research has been mainly to define the characteristics of older cancer patients, analyze how they were tolerating cancer treatments, and how to best integrate geriatric tools and expertise (mostly the CGA) into cancer care.
The following concepts are presently under very active investigation:
-A two steps approach to the initial evaluation of older cancer patients is becoming the paradigm of choice. A short screening tool applied in the oncology practice, followed by a more comprehensive geriatric assessment and an integrated approach by a multidisciplinary team for those who screen positive. A range of short screening tools are becoming available for use (see below).
-The integration of geriatric instruments as decision tools in the treatment of cancer. At this year's ASCO meeting, two scores for predicting toxicity from chemotherapy were presented (4,5). These are only the most prominent of a host of efforts at defining robustness or frailty when it pertains to cancer treatment.
In addition, some concepts are going to take an increasing importance in the near future:
-Comorbidity is increasingly recognized as more than an independent bystander. Comorbidity and its treatment appear to influence the behavior of the cancer itself (e.g. cancer risk, risk of relapse, response to treatment (6,7)). Therefore it will need to be integrated into management decisions to an even higher degree than it is now. For example, as diabetics relapse more frequently from a colon cancer (8), should we offer adjuvant chemotherapy to all diabetics with stage II colon cancer?
-Individualization of pharmacokinetics/pharmacodynamics of cancer drugs. Older patients present a high variability in body composition and organ function. They are a prime population for individualized drug adjustment. While useful, pharmacogenomics may only be part of the answer, as older patient for example take multiple medications. Rapid methods assessing plasma levels of drugs, p450 function, or protein binding may all become useful in clinic.
-It is also important to develop effective models of cooperation between geriatricians and oncologists. The biologic interaction between aging and cancer is also a rich source of potential development. Most of our animal models have been so far geared toward young animals. Yet senescence brings important changes and taking it into account might lead to more successfully translatable results. Cancer and its treatment could also be used as a stress model to understand adaptative/biological aging. In aging research, cancer could provide a great model of studying aging organisms under stress. Since the decrease of functional reserve, rather than baseline functioning, is the major change of aging, it could best be studied in someone with a chronic disease such as cancer. As the treatments also have a few months duration, they can offer a model of additional short duration stress.
Specific Research Areas
1. Patient profile
One of the first challenges faced by academic oncogeriatricians was to define the profile of older cancer patients. What was their level of comorbidity? How selected were they compared to other older patients? We now have profiles for several populations: Oncologic outpatient clinics, oncologic inpatient units, geriatric outpatient clinics and inpatient geriatric evaluation and management units (GEMU), and population databases (Table 1). Some overall remarks can be made. Whereas cancer patients tend to be healthier than their counterparts, they still carry a strong burden of comorbid conditions, even in tertiary centers. Also, there are clear similarities in the profile of patients from different countries. We have also learned that, while social expectations toward treatment of older cancer patients may differ, cancer patients in Europe and America are strikingly similar in their willingness to undertake treatment (9). Data on Asian populations are still scarce.
Large epidemiologic studies have explored various aspects of cancer in the older person. American studies have mostly used the SEER/Medicare database, and European studies have tapped either national or European registries (e.g. (10-14)). They have demonstrated a general pattern of undertreatment of older patients. This pattern is not clearly explained by comorbidity, although some degree of correlation exists. They also demonstrated that this undertreatment had a prognostic impact.
An increasing number of patients survive their cancers. As they age, these cancer survivors have a significant likelihood of developing second cancers. In a retrospective analysis of Floridian patients, 20% of them had two cancers or more (15). Epidemiologic studies could clarify time relationships and associative patterns of these multiple cancers. Another aspect where epidemiology will be instructive is the analysis of the impact of prevention measures in adulthood. As a wider population is on statins or NSAIDS for prevention of cardiovascular disease, this is likely to impact significantly on the epidemiology of cancer in the elderly. As smoking cessation efforts increase, this will have an impact on late life cancers as well. Will the number of cancers simply decrease, or will smoking-related tumors be replaced by others? The very old are also the fastest growing segment of the US population. By 2050, the US Census bureau estimates there will be about 1 million centenarians living in the US (16). Right now, the incidence of cancer appears to decrease after age 85. Whether this is due to under detection, or a protective action of longevity genes is unclear. This should clarify in a near future. If the latter is true, then the epidemiology of geriatric oncology could be a powerful tool in the development of genetic epidemiology, as tools such as human genome mapping become more widely available. We could develop studies of familial cancer resistance syndromes as a counterpart to familial cancer syndromes. A longitudinal cohort study is already beginning to identify cancer patterns in centenarians (14). Epidemiologic databases have made progress into integrating more and more comorbidity. Some databases, such as the NCCN breast database, also include functional status information. Other databases include treatment information (e.g. Medicare, NCCN). Sophisticated databases with comorbidity, functional, treatment and genetic information is being developed by some centers (for example Moffitt's Total Cancer Care database). This is a potential gold mine to study prognostic interactions in patients with multimorbidity.
2. Geriatric assessments and interventions
Given the high comorbidity burden cancer patients carry, and the demonstrated effectiveness of CGA in general, researchers started integrating a CGA in their clinics and studies. Whereas clinic practices are highly setting-dependent, some patterns have emerged in research assessments. The dimensions measured are functional status, both with oncologic instruments and geriatrics instruments (ADL/IADL), depression, cognition, nutrition, and physical performance (17-22). An increasing amount of data demonstrates, in a rather constant fashion, an independent predictive effect of IADL, ADL, depression, comorbidity and cognitive status, independently from classic oncologic and surgical prognostic factors such as EGOG PS or the ASA score (17,21-27). What is now needed is a functionalization of these instruments for decision-making in geriatric oncology. A few studies have focused on geriatric interventions in cancer patients. The largest one is a study of a one month geriatric intervention in post-operative cancer patients (28). Whereas the intervention was not making a difference in patients with early stage disease, it strikingly increased the survival at two years of patients with advanced stage by 27% (67% vs 40%). Another study demonstrated that CGAs repeated every 3 months in early breast cancer patients were detecting a significant amount of untreated problems. On average, 6 problems per patient were found at baseline, and an additional 3 problems were detected over the ensuing 6 months (29).
More recently, the focus has turned to a two-step approach. Many groups are trying to develop a short screening tool that could be applied easily in an oncology practice to select patients for further comprehensive evaluation (30-35). It appears that about half of patients 70 and older are needing such a referral (30,36). Our group uses the SAOP2 screening tool (37), but several tools, such as the VES 13, the TRST, and others are being actively tested. This is a rapidly evolving research field.
3. Treatment patterns and tolerance
Several epidemiologic studies have explored the treatment patterns of older cancer patients and their consequences. There seems to be clearly an age effect beyond the impact of comorbidity (e.g. (38-40)). Some of the earliest studies were retrospective analyses of cooperative group studies. Older patients are underrepresented in such studies. However, the selected elderly who are enrolled tend to derive a similar benefit from their treatment, at the cost of a similar or somewhat higher toxicity (41). An aspect where much less data is available is response and toxicity patterns of patients in intermediate condition that would not fit standard study inclusion criteria, or studies addressing the general population of oncology clinics. Two studies prospectively assessed such a population (18,42). One observed 60 patients with various cancers. It identified a rate of grade 4 hematologic or grade 3~4 non-hematologic toxicity in half of the patients (18). Yet most were able to complete their treatment with little impact on their functional status (43). The other study focused on breast cancer patients (42). Here again, half of the patients experienced toxicity but were able to continue. Two large studies recently reported on predictive scores for the risk of severe side effects from chemotherapy. The first one is the CRASH score (Chemotherapy risk assessment score for high-age patients), built by our group in 518 patients (4). It aims at predicting Grade 4 hematologic toxicity and/or grade 3~4 non-hematologic toxicity. The second one is a score designed by Dr Hurria and the Cancer and Aging Research Group (5). It aims at predicting the risk of Grade 3~4 toxicity (hematologic or non-hematologic). They are available from their first authors upon request, pending their full written publication.
4. Clinical protocols
Underaccrual of elderly patients into cooperative clinical trials is a challenge. Complex physician- and patient-related factors are involved. Several studies have helped understand these challenges (44-46). One randomized study by CALGB devised an intervention to remedy this problem, but unfortunately was unsuccessful (47). A model suggest that the best success rate could be achieved by designing "comorbidity-tolerant" studies (48).
Several therapeutic trials have focused on the elderly. The tumors in which we have learned the most so far are high-grade non-Hodgkin's lymphoma and non-small cell lung cancer (NSCLC). A series of studies in the early nineties explored whether anthracyclines could be spared in the treatment of older patients with diffuse large cell B-cell lymphoma. The conclusion was that standard dose CHOP remained the standard in elderly patients (49). The addition of rituximab is likewise beneficial in older patients. In fact, the older patients appear to benefit most from the addition of rituximab (50). Several studies also demonstrated that the administration of CHOP-like regimens should be accompanied by the prophylactic use of neutrophilic growth factors from the first cycle on (51,52). More recently, two studies explored the use of lower dose regimen in frail elderly who were not candidate for CHOP (20) (Soubeyran et al. personal communication, SIOG 2005). Although response rate and survival were lower, a third of these frail patients were still alive at 1 year. It should be noted that in that group of patients, the occurrence of a severe toxicity often has dire consequences.
In NSCLC, four randomized studies have explored the use of chemotherapy in the elderly (53-56). The ELVIS trial demonstrated that single agent vinorelbine increased survival and quality of life over best supportive care (53). Two other studies led contradictory results as to whether the combination vinorelbine and gemcitabine was better than either alone (54,55). A study presented at this year's ASCO Plenary Session demonstrated that carboplatin-paclitaxel was more effective than single agent chemotherapy in patients 70 years and older (56). It is interesting to note that studies specifically targeting the elderly indeed recruit older patients than parallel general studies (57). 17% patients were in their eighties, whereas only 3% of patients were in that age range in the other studies.
Many hematologic studies are being conducted in patients above 60, i.e. not transplant candidates. They mostly recruit young elderly patients. Some randomized adjuvant breast cancer studies focusing on women 65 years and older have been published (58,59) and others are in progress. Studies are being conducted in various other cancers as well.
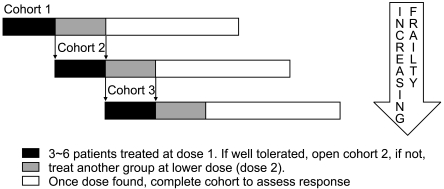
The major challenge of geriatric oncology for the years to come will be to broaden the accrual of older patients into clinical trials. Innovative trial designs need to be found to allow the inclusion of patients with multiple comorbidities into formal therapy assessments in a safe matter. One example could be a progressively increasing inclusion criteria (PIIC) design. A PIIC design could adopt a format similar to a phase I/II trial, where instead of increasing the dose of the drug, we broaden the inclusion criteria in a controlled fashion, adjusting the regimen for toxicities. That can be followed by the multilevel phase II part, where we compare the outcome of the different comorbidity subgroups (Fig. 1). Trials could also be designed specifically for various subsets of older patients, such as the vulnerable or the frail elderly, as some studies have started doing (e.g. (20)).
The definition of vulnerable and frail elderly cancer patient needs to be clarified. It may or may not be the same as in other geriatric settings. The trial designs above could help in that process. Another strategy with a great potential is to incorporate geriatric instruments as stratification tools into trials. In other words, to take them from their demonstrated prognostic correlations to the next step of being decision helps. The two most mature candidates for that role are comorbidity and IADL. Many vulnerability/frailty definitions are also being tested in geriatrics and would warrant parallel testing in older cancer patients.
5. Decision-making
Several projects used decision-making methods to incorporate comorbidity and other variables in the treatment of older cancer patients. One of the first topics being addressed was the adjuvant treatment of older breast cancer patients (60). This type of approach to comorbidity has since been integrated in widely used tools such as Adjuvant! (http://www.adjuvantonline.com). Another model addressed the use of surgery and radiation therapy in older men with early prostate cancer (61). Models have also been used to address the issue of mammography screening in older women, notably its cost-effectiveness as age increases, and the selection of a subpopulation that would benefit most from it (62,63). As desirable as studies for as large as possible a range of health conditions in elderly patients are, they will never cover every possible case scenario older patients can present with. Therefore decision models clearly have a role. They do not however replace proper studies, as they rely on study generated data and the more data available, the more precise the models will be.
6. Biology of cancer and aging
Several laboratory and translational studies have explored the modification of the biology and behavior of cancer with age, as well as concepts such as the antagonistic pleiotropism of aging and cancer (64-67). This is an emerging field. A tremendous effort has been invested into understanding the biology of cancer since the 1970s. More recently, the biology of aging and senescence has also made significant progress. I see the convergence of these two areas of research as having great development potential for the cancer and aging research. This research has also demonstrated that the mechanism of action of cancer vaccines changes with age (68). I believe that an increased interaction between aging and cancer researchers could help focus drug development on critical pathways. Another way that could lead to more effective screening of cancer drugs is the use of old animal models. Most in vivo animal studies are conducted on 6~8 week old mice, the equivalent of teenage humans. These mice are at the peak of their immunity and tumor prevention or shrinkage can be quite readily induced. However, many drugs tested in these models prove ineffective when tested in phase I studies. Part of the problem may be the difference in age of the test populations. My postulate is that if the step were taken of duplicating the results in old animals before going to humans, we might select out marginally effective drugs and spare ourselves the cost of human phase I trials with them.
7. Translational research
Many aspects of aging and cancer can be addressed by translational research. One aspect, as mentioned above, is cancer as a stress model in older adults to better understand biological and physiological aging. Another aspect is the understanding of the interactions between comorbidities and cancer at the biologic level and design counter-measures. This is a rich and yet relatively untapped area of research. Good examples of that would be diabetes or metabolic syndrome and cancer, or obesity and cancer. A tantalizing avenue of translational research is the investigation of cancer-resistant families. The number of the oldest old increases rapidly. The rate of incidence of cancer appears to decrease after the age of 85. Therefore mapping the genome of very old representatives of cancer-free families might help discover a series of anti-oncogenes and longevity genes (or epigenetic phenomena) that could be exploited in cancer prevention and treatment.
8. Prevention and screening studies
So far, very little work has been done on the prevention and screening of cancer in the elderly. For example, randomized studies of screening mammography included very few women above the age of 70 and none over the age of 75. Yet an average 75 years old woman still has 10 years of life expectancy, and screening efforts should not be considered a priori futile. As carcinogenesis is a multistep process that can evolve over decades, cancer prevention in the elderly should by necessity target late events in carcinogenesis. If we target these events, then it is worth noting that prevention efforts that would reduce, say, the 5 years incidence of cancer (or its recurrence), would benefit a large number of elderly subjects. Therefore there is clearly a role for prevention studies in the elderly.
Program Developments and Clinical Practice
Research is of course of little benefit to the patient if not applied. Therefore, geriatric oncology programs are emerging with increasing momentum around the world. The first programs dedicated to geriatric oncology appeared in the mid-nineties in places such as Tampa, Aviano, or Lyon. These programs started to work out the first forays in the integration of geriatrics and oncology. As they demonstrated the prevalence of complex pathologies, the interest grew, and by the turn of the millennium, various organizations, such as the Hartford Foundation, then ASCO, started supporting the training of young geriatric oncologists. In the first decade of this millennium, governmental efforts were conducted to develop programs, for example by the American National Institutes of Health (NIH), which funded grants to develop geriatric oncology programs, or the French National Cancer Institute (INCa) that has funded the development of geriatric oncology units in each main region of France. Several continuous education courses have been set up, not only in developed countries, but also in areas such as the Middle East or India. Textbooks and curricula are now available (examples: (69-73)), and geriatric oncology is making its way into general cancer guidelines, such as the NCCN guidelines (www.nccn.org). Increasingly, large cancer centers develop integrated geriatric oncology programs, some hiring geriatricians or dual trained geriatric oncologists into the center. Others harness the multidisciplinary environment of their university with collaborations of the geriatric and oncologic teams.
The impact of cancer in the elderly is bound to be a worldwide phenomenon. In about 20 years from now, there will be more patients aged 65 and over in India than in the USA. The proportion of older people will be between 10 and 30% in most countries, which means more than 1 billion worldwide. A quarter to a third will be expected to develop a cancer, i.e. 250~300 million people. The only way we can develop adequate care for that number of patients is to use a "train the trainer" approach. We will need to develop a cadre of geriatric oncology specialists (dual-trained or multidisciplinary teams), committed to research and teaching in this particular field. Geriatric oncology specialists will train their geriatrics and oncology colleagues, who in turn will form trained teams in their institutions. These local institution-based teams will train the private practice colleagues in their area. Institutions and private practices will need to develop multidisciplinary structures to treat what already is and increasingly will be a major part of their patients. It is estimated right now that in tertiary centers half of the older cancer patients are in need of a comprehensive oncogeriatric approach (36). These structures will need to include not only oncologists and geriatricians, but also a team of social workers, dieticians, physical therapists, pharmacists, nurses and mid-level practitioners with knowledge pertaining to this patient population.
SIOG and Other Societies
An international society, the International Society of Geriatric Oncology (SIOG, from the French version of the name), was created in 2000 to promote the development of geriatric oncology worldwide. It has already produced several recommendations and guidelines for the care of older cancer patients ((74,75) and www.siog.org). Its annual meeting has also proven to be a great opportunity for interactions among researchers in the field. I see this Society and other national societies as a catalyst of the development of geriatric oncology training, research and practice around the world. Medical Oncology Societies are also paying increasing attention to the older cancer patients. For example ASCO developed a syllabus in geriatric oncology (69) and ESMO and SIOG just published a handbook of geriatric oncology (71). The ASCO, ESMO (European Society of Medical Oncology), and AGS (American Geriatrics Society) annual meetings have all featured geriatric oncology sessions.
Conclusion
Geriatric oncology is now growing beyond its pioneer years. The speed at which scientific data accumulate is increasing, providing an increasingly solid background for the individualized care of the older patient, although a long road remains ahead. As a group of specialized practitioners and researchers is emerging and the patient population is increasing rapidly, the next ten years will no doubt produce major progress in this area. Geriatric oncology is going to become a major component of oncology and geriatric practice, and therefore appropriate consideration and support to it will need to be developed in public health, institutional and educative policies around the world.