Introduction
Eosinophils are derived from multipotent and lineage-committed hematopoietic stem cells [1]. The major growth factors for eosinophils are interleukin (IL)-3, IL-5, and granulocyte monocyte-colony stimulating factor (GM-CSF). These regulators are produced by activated T lymphocytes, mast cells, and tissue stroma cells [2,3]. Peripheral blood eosinophilia is defined as an absolute eosinophil count (AEC)≥0.5×109/L. The degree of blood eosinophilia is classified as either mild (AEC, 0.5×109/L to 1.5×109/L), moderate (AEC, 1.5×109/L to 5.0×109/L) or severe (AEC,>5.0×109/L) [3,4].
In general, eosinophilia is divided into either familial or acquired types. Acquired eosinophilia is classified as primary or clonal eosinophilia (based on the presence of histological, cytogenetic or molecular markers of a myeloid malignancy in the bone marrow), secondary eosinophilia (a cytokine-driven reactive phenomenon), and idiopathic eosinophilia (neither secondary nor clonal), which includes idiopathic hypereosinophilic syndrome (HES) [3,4]. The causes of secondary eosinophilia are infections (mostly helminthic), drugs, pulmonary eosinophilia, autoimmune diseases, inflammation, endocrinopathies, and malignancies [2-4]. Both hematopoietic and solid neoplasms may be associated with peripheral blood eosinophilia [3,5]. However, there have been few reports on the association between multiple myeloma (MM) or plasma cell disorders and eosinophilia, and the few cases that have been reported have found outcomes after chemotherapy to be poor [6-8].
We now report a case of a 31-year-old male with MM who had marked absolute peripheral blood and bone marrow eosinophilia, leading to multiple organ dysfunction with eosinophil infiltration. After chemotherapy followed by autologous stem cell transplantation (ASCT), the patient achieved complete remission (CR).
Case Report
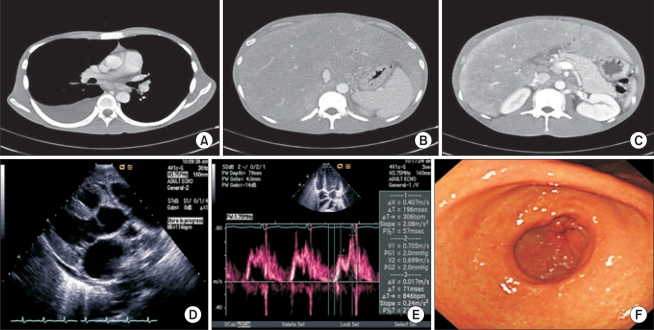
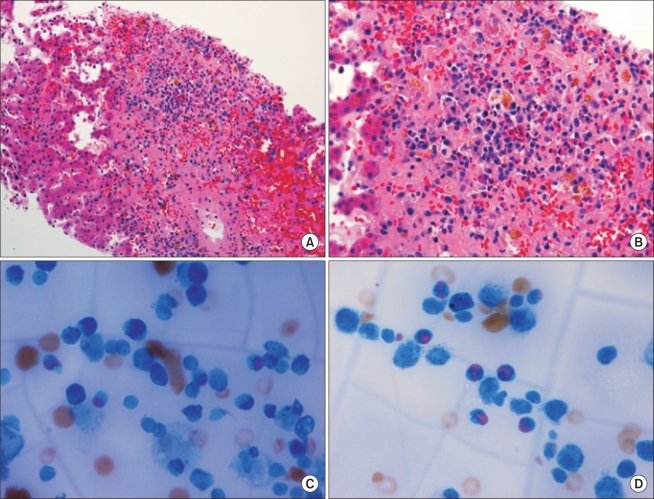
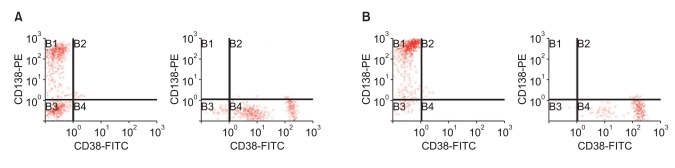
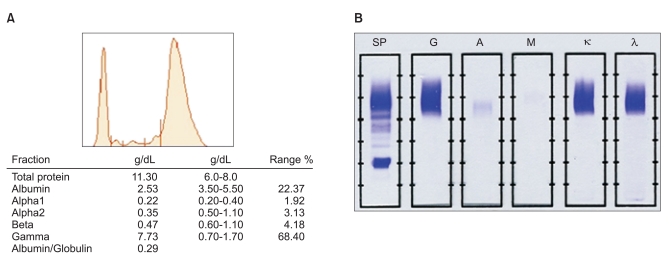
A 31-year-old man was hospitalized for fever, fatigue, and abdominal discomfort. He reported no recent travel history, there was no history of urticarial or other allergic symptoms, and he had no history of alcoholism. Vital signs at the time of admission were as follows: temperature, 38.3℃; pulse, 92 beats per minute; blood pressure, 125/75 mm Hg; and respiratory rate, 18 breaths per minute. The initial physical examination revealed hepatosplenomegaly, a distended abdomen with ascites and significant pitting edema in both lower limbs. An initial complete blood count (CBC) found a hemoglobin (Hb) level of 8.3 g/dL, a white blood cell count (WBC) of 12,300/µL and a platelet count of 77,000/µL. A differential WBC showed 36% neutrophils (4,430/µL), 28% lymphocytes (3,440/µL), and 35% eosinophils (4,310/µL), but did not include circulating myeloid precursors or other left-shifted neutrophils. The patient had also suffered from eosinophilia eight months previous (Hb, 13.4 g/dL; WBC, 8,590/µL [eosinophils, 2,233/µL]; platelet count, 203,000/µL). Other laboratory findings were as follows: lactate dehydrogenase, 496 IU/L; protein, 12.7 g/dL; albumin, 2.2 g/dL; IgE,>3,000 IU/mL; IgG,>5,000 mg/dL; IgA, 152.7 mg/dL; IgM, 162.8 mg/dL; Bence-Jones protein (+); β2-microglobulin, 4.70 mg/L; serum vitamin B12 level, 1,428 pg/mL; folic acid level, 2.91 ng/mL; serum free kappa light chain, 566.0 mg/mL; serum free lambda light chain, 765.0 mg/mL; anti-nuclear antibody (-); anti-double strand DNA antibody (-); anti-mitochondrial antibody (-); hepatitis B virus surface antigen (-); and anti-hepatitis C virus antibody (-) (serum tryptase was unavailable for testing). Bone marrow aspiration and biopsy showed hypercellular marrow with high levels of eosinophilic (19.1%) and plasma (22.9%) cells with no increases in other matured myeloid precursors (Fig. 1). A chromosomal study was normal (46, XY), and fluorescence in situ hybridization (FISH) analyses for platelet-derived growth factor receptor (PDGFR) and BCR/ABL were negative. Our diagnostic evaluation of the eosinophilia included a stool specimen negative for parasitic infection and a negative multiple antigen simultaneous test (MAST). A computed tomography (CT) scan of the chest showed effusion of the right pleura (Fig. 2A). Abdominal CT revealed hepatosplenomegaly of both hepatic lobes without a definite focal lesion, fluid in the perihepatic space and lymph node enlargement in the peripancreatic, mesenteric, and aortocaval areas (Fig. 2B and C). An echocardiogram showed minimal pericardial effusion, septal hypertrophy and mild global hypokinesia of the left ventricle (Fig. 2D and E). Endoscopy found diffuse-fashioned erythema of the stomach mucosa in the antrum (Fig. 2E). We could not perform a biopsy of the heart or stomach because the patient was prone to complications from invasive procedures (e.g., excessive bleeding and pleural effusion). A liver biopsy showed parenchymal infiltration of numerous eosinophils and plasma cells on the hemorrhage focus (Fig. 3A and B). Plasma cell markers were positive in the peritoneal (CD138, 60.12%; CD38, 96.2%) and pleural (CD138, 96.18%; CD38, 99.8%) fluids (Fig. 4). The cytology results of the ascites and pleural fluids showed plasma cells and eosinophils (Fig. 3C and D). Based on these results, eosinophilia involving the bone marrow, liver, and lungs was confirmed, and eosinophilia involving the peritoneal cavity, heart, and stomach were considered possibilities. Moreover, the patient's albumin/globulin ratio was reversed. A monoclonal peak was observed in the gammaglobulin fraction from serum protein electrophoresis (Fig. 5A), and immunofixation electrophoresis revealed IgG, kappa and lambda paraproteins (Fig. 5B). Therefore, the patient was diagnosed with MM with biclonal gammopathy. Three weeks after starting dexamethasone, the patient was treated with a bortezomib (Velcade®, Ben Venue Laboratories, Inc., Bedford, OH) plus dexamethasone (VD) regimen every three weeks. Four months following the start of the VD regimen, the patient's laboratory findings improved. The patient then underwent ASCT. His treatment was maintained (with thalidomide plus dexamethasone) for six months after ASCT. Currently, he has finished treatment and has been followed-up with laboratory tests for nine months. A recent CBC revealed an Hb level of 14.1 g/dL, a WBC of 4,100/µL with a differential cell count of 10% eosinophils (410/µL) and a platelet count of 127,000/µL. The eosinophil count of the patient did not exceed 1.5×109/L on consecutive readings after initiation of ASCT. Other laboratory findings included an IgG concentration of 1,085 mg/dL, serum free kappa/lambda light chain of 16.60/17.60 mg/mL, a kappa/lambda ratio of 0.94, and negative immunofixation and β2-microglobulin of 1.70 mg/L. The laboratory findings were all in normal ranges. He is now in a status of CR for MM. His liver and spleen have decreased in size, and they and other organs have recovered their functionalities.
Discussion
A wide variety of solid tumors (predominantly carcinomas of the lung, head and neck, uterus, breast, pancreas, colon and rectum, thyroid gland, adrenal glands, and the biliary tract) may be associated with eosinophilia [5,9]. A number of lymphoid neoplasms may be accompanied by eosinophilia, including Hodgkin's disease and T-cell lymphomas and, less frequently, B-cell non-Hodgkin's lymphomas, natural killer cell neoplasms, and other B cell malignancies [2,3,5]. There have been some case reports of eosinophilia associated with lymphoid malignancies [10,11]. However, there have been few reports on eosinophilia with MM or plasma cell disorders [6,7]. In Korea, only one case has been diagnosed as chronic eosinophilic leukemia with MM [8]. In our case, primary and clonal eosinophilia were excluded based on the results of FISH and chromosomal studies, and myeloproliferative disease was ruled out based on the absence of circulating myeloid precursors and normal chromosomal and bone marrow findings, without a left shift in maturation except for eosinophils and plasma cells. In Japan, a case of MM and chronic hepatitis C has been reported [12]. According to the laboratory findings of our case, the patient did not have a chronic liver disease. We diagnosed secondary eosinophilia associated with MM because the patient had an eosinophilia-concomitant hematologic malignancy. There is no acceptable mechanism to explain the occurrence of peripheral blood eosinophilia in patients with plasma cell disorders. Stefanini et al. [13] suggest four hypotheses. First, the release of a protein from necrotic tumor cells may result in eosinophilia. Second, the presence of a metastatic tumor in the bone marrow may stimulate eosinophilopoiesis. Third, eosinophilia may represent a genetic or familial response to malignant tumors. Finally, neoplastic cells may actively secrete substances that either directly or indirectly (via secretion by other cells) result in eosinophilia [13]. According to Stefanini et al. [13], IL-3, IL-5 and GM-CSF promote eosinophilopoiesis in patients with hematologic malignancies. However, we could not study these relationships in our case, because IL-3, IL-5, and GM-CSF levels were not measured in our patient.
In our case, biclonal gammopathy was noted (Fig. 5B). There have been few reports on MM with biclonal gammopathy, and its incidence is about 1% of all monoclonal gammopathies. MM with biclonal gammopathy is associated with malignant lymphoma [14].
Imatinib is the standard treatment in patients with clonal eosinophilia including PDGFR mutations, and cytoreductive therapy or steroids are the treatments of choice with HES. Secondary eosinophilia can be addressed by treating the underlying disease. Drug-refractory eosinophilia is usually treated with chemotherapy and allogenic stem cell transplantation [2,4,9,15]. The main therapy for plasma cell disorders with eosinophilia has been melphalan, vincristine, adriamycin and dexamethasone (VAD) or cyclophosphamide [6,7]. The majority of these published cases did not achieve sustained responses, and plasma cells or eosinophils increased in the bone marrow or the peripheral blood of these patients shortly after termination of the treatment. Life expectancies in these cases were short.
At present, there is no standard treatment for patients with MM and eosinophilia despite the poor response and prognosis. Even though there are no reports that suggest treatment via hematopoietic stem cell transplantation in cases similar to ours, we performed ASCT after induction chemotherapy with a VD regimen. Through this treatment, our patient achieved CR of at least six months without other therapies. Long term follow-up is required to confirm the sustained response.