Introduction
Urothelial carcinoma (UC) is the seventh most common malignancy in Korean males. According to the Korea National Cancer Incidence Database, 10.4 per 100,000 Korean males suffered from UC in 2008 [1]. Approximately 20% of cases of bladder cancer are clinically advanced at presentation, and many patients with superficial or locally invasive disease eventually develop metastases. Thus, management of advanced UC is a much more common problem than would be inferred from published incidence rates [2].
Chemotherapy is the treatment of choice for metastatic UC. Cisplatin-containing combination chemotherapy such as gemcitabine and cisplatin (GC), may achieve excellent response rates, especially in patients with lymph-node metastases only, good physical status, and adequate renal function, including a complete response in up to 20% of patients achieving long-term, disease-free survival [3]. However, at the present time, there are insufficient data to provide a recommendation on standard second-line chemotherapy [4]. Unfortunately, patients frequently experience significant deterioration of the performance status, renal function, or both with disease progression after first-line treatment. Thus, these patients are not candidates for further systemic chemotherapy [5]. In recent years, a clinically evident stage migration has led to earlier detection of metastatic disease. Concomitantly, use of neoadjuvant and adjuvant chemotherapy has increased, resulting in an increased proportion of patients who are fit enough for second-line chemotherapy for metastatic disease [6]. Several single-agents have recently been investigated for second-line chemotherapy in phase II clinical trials, including ifosfamide, taxanes, ixabepilone, gemcitabine, pemetrexed, and vinflunine. In these studies, response rates have ranged between 8.6% and 27.7% [7,8,9,10,11,12]. However, none of these drugs has been accepted as standard second-line chemotherapy.
Methotrexate, vinblastine, doxorubicin, and cisplatin (MVAC) was the standard chemotherapy regimen prior to GC [13]. Despite its significant clinical efficacy, MVAC was replaced by GC because GC has a better toxicity profile in terms of leucopenia, mucositis, and neutropenic fever [14]. A dose variant of MVAC has been reported to have higher efficacy than the original regimen with tolerable toxicity [15]. Thus, we replaced adriamycin with epirubicin, and omitted methotrexate and vinblastine on day 22 in order to improve the toxicity profile. In this retrospective study, we evaluated the efficacy and toxicity of modified MVAC in patients for whom GC failed.
Materials and Methods
1. Patients
A total of 28 patients with metastatic urothelial cell cancer who had previously been treated with a GC-containing regimen received MVAC as salvage treatment at the Korea University Medical Center, Seoul, South Korea between November 2004 and November 2012. All patients were pathologically confirmed with metastatic urothelial cell cancer and had adequate hematologic parameters (absolute granulocyte count≥1,500/dL, hemoglobin≥9 g/dL, and platelet count ≥ 100,000/dL), adequate hepatic functions (serum total bilirubin<1.5 mg/dL, transaminases<2× the upper limit of normal), and renal function (estimated glomerular filtration rate≥60 mL/min). The following clinical data were collected from the medical records of each patient: physical examination, surgical and pathological reports, and imaging reports. Medical information, including chemotherapy regimens; dose of cytotoxic agents; response; toxicity profile; and the dates of progression, last follow-up, and death were collected. Signed, informed consent was obtained from all patients before treatment, and this study was approved by the Ethics Committee of the Korea University Medical Center (KUMC).
2. Chemotherapy
A dose of 30 mg/m2 methotrexate was administered by intravenous (IV) infusion on days 1 and 15. A dose of 3.0 mg/m2 vinblastine was administered IV on days 2 and 15. Doses of 30 mg/m2 epirubicin and 70 mg/m2 cisplatin were administered IV on day 2. The cycle was repeated every 28 days. Treatment continued until toxicity was intolerable or the disease progressed.
3. Evaluation of efficacy, toxicity, and dose modification
Evaluation of response, toxicity, and modification of dosage was performed according to local practice guidelines. Briefly, computed tomography (CT) scans of target lesions were performed every eight weeks and repeated CT scans were performed for evaluation of subsequent responses. Responses were classified according to response evaluation criteria in solid tumor guidelines (ver. 1.1) [16]. Before starting each cycle, toxicity was graded according to the National Cancer Institute Common Toxicity Criteria (NCI CTC) ver. 4.0.
The dose was reduced in patients who experienced grade 4 hematologic or grade 3/4 non-hematologic adverse events. The dose was not re-escalated after it was reduced. Modified MVAC was delayed up to two weeks in the case of significant hematological or non-hematological toxicity.
4. Statistical analysis
Descriptive statistics were used for characterization of patient demographics, response and toxicity rates, and laboratory observations. Overall survival (OS) was calculated as the time between the start of treatment and death or the last follow-up. Progression-free survival (PFS) was calculated from the first day of chemotherapy until progression or the last follow-up for any other reason. PFS and OS curves were obtained using the Kaplan-Meier method. All statistical analyses were performed using the SPSS ver. 12.0 (SPSS Inc., Chicago, IL). Response duration was calculated from the date of response confirmation to the date of disease progression.
Results
1. Patient characteristics
A total of 28 patients were treated with this chemotherapy regimen at the Korea University Medical Center between November 2004 and November 2012. All patients failed in prior, first-line chemotherapy with GC. In first-line GC chemotherapy, the median number of chemotherapy cycles was 3 (range, 1 to 8). The median treatment-free interval between GC and modified MVAC was 26 weeks (range, 3 to 168 weeks).
There were 21 males and seven females and the median age of patients was 64.0 years (range, 33.0 to 77.0 years). Twenty three (82.1%) patients had an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. The bladder (64%) was the most common primary site. All patients had metastatic, locally advanced or recurrent UC. The median number of metastatic sites was 2 (range, 0 to 3). Lymph node (26/28, 93%) was the most common metastatic site, followed by the liver (11/28, 39%) and lung (6/28, 21%). Characteristics of patients and disease are shown in Table 1.
2. Response
Of the 28 patients included in this study, three were excluded from the response analysis due to refusal refusal to undergo imaging studies. Data on the treatment efficacy are shown in Table 2. Response rates were calculated in the intent-to-treat population. A partial response was observed in nine patients (36.0%), and stable disease was observed in seven (28.0%). The disease control rate was 64.0 %. Nine patients (36.0%) had progressive disease. Overall, disease control was achieved in 61.9% of patients who responded to first-line GC treatment. The median response duration was 19 weeks (range, 6 to 90 weeks).
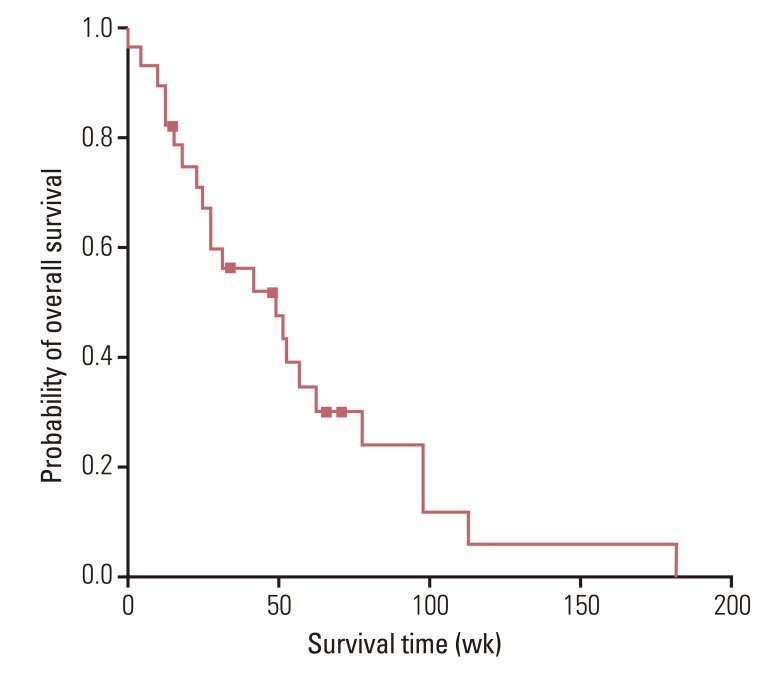
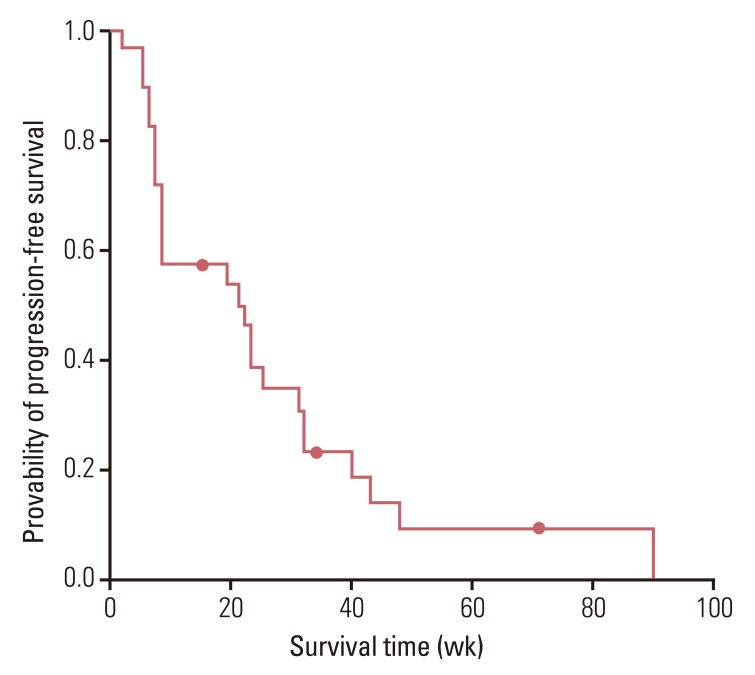
3. Survival
Overall, 25 patients were included in the survival analysis. The median duration of follow-up was 38 weeks (range, 5 to 182 weeks). At the time of analysis, 22 patients had died, one patient was alive after disease progression, one stopped taking treatment after obtaining a response, and four were under treatment. The median OS was 49.0 weeks (95% confidence interval [CI], 18.8 to 79.3 weeks), and the median PFS was 21.0 weeks (95% CI, 6.3 to 35.7 weeks). OS and PFS are shown in Figs. 1 and 2.
4. Toxicities and dose reductions
A total of 28 patients received 101 cycles of treatment. The median number of cycles administered was 3 (range, 1 to 8). A list of the toxicities observed in this study is shown in Table 3. The major hematological toxicity was neutropenia. Nine patients (32.1%) experienced grade 3 or 4 anemia (13.9% of cycles), and 21 (75.0%) experienced grades 3 and 4 neutropenia (42.6% of cycles). Four patients experienced febrile neutropenia. The incidence of thrombocytopenia was low; three patients (10.7%) developed grade 3 thrombocytopenia (3.0% of cycles). Non-hematological toxicities were not severe and were reversible; renal toxicities (60.7% of patients) and anorexia (25% of patients) were all grade 1 or 2. There was no treatment-related mortality in this study population.
Discussion
Metastatic UC is sensitive to chemotherapy, and a cisplatin-based combination regimen (GC) is the standard first-line treatment. GC is preferred to MVAC due to its lower toxicity with comparable efficacy [17]. Although the overall response rate of cisplatin-based therapy ranges from 50% to 70%, nearly all patients experience disease recurrence within the first year. The median survival time is approximately 12-14 months [13,18,19]. In addition, the overall clinical condition shows significant deterioration, often in association with renal impairment after progression following first line chemotherapy. De Wit [20] reported that an estimated one-third of patients with advanced UC are medically unfit for cisplatin-based chemotherapy. Therefore, single agents and non-cisplatin-based combination chemotherapy have been investigated in clinical trials for prevention of cisplatin-induced nephrotoxicity. So far, use of a single agent, ifosfamide, taxane, ixabepilone, gemcitabine, pemetrexed, or vinflunine, after cisplatin-based therapy has resulted in response rates of 8.6-27.7%, however, OS did not show improvement [7,8,9,10,11,12]. A non-cisplatin doublet, combined paclitaxel and gemcitabine, the most extensively studied second line regimen, has been shown to be effective in treatment of patients with advanced UC and had lower toxicity (odds ratio [OR], 33.3%; OS, 11.3 months) [21].
However, a recent study showed that cisplatin-based therapy is reasonable for second-line chemotherapy. Han et al. [22] studied the efficacy and toxicity of MVAC as a second-line systemic chemotherapy for patients who had progressed after GC2121. Standard MVAC resulted in an overall response rate of 30%, a median PFS of 5.3 months, and a median OS of 10.9 months. Patients who previously responded to GC chemotherapy had better response rates. Findings of this study suggest that cisplatin may be active in patients who fail the GC protocol and that metastatic urothelial cancer may be sensitive to other agents, such as methotrexate, doxorubicin, or vinblastine. However, standard MVAC in a second-line setting still produced significant toxicity, such as neutropenia, thrombocytopenia, mucositis, and alopecia. Although standard MVAC had moderate efficacy, a safer combination is necessary for patients who progress after failure of first-line chemotherapy.
In the current study, MVAC was adjusted for treatment of patients with a deteriorated physical state, depleted bone marrow reserves, and impaired renal function after failure of first-line chemotherapy. To improve tolerance, methotrexate and vinblastine were omitted on day 22, and 30 mg/m2 epirubicin was used instead of 30 mg/m2 doxorubin in order to reduce the dose by 1.5-fold. Use of this modified MVAC schedule as a second-line chemotherapy resulted in a moderate response rate (OR, 36.0%) with a survival time comparable to that of standard MVAC (PFS, 21.0 weeks; OS, 49.0 weeks). Correlation was observed between the response to first-line GC and the response to modified MVAC, which was observed in the previous study using standard MVAC. Overall, Disease control was achieved in 61.9% of patients who responded to first-line GC treatment. Response rates in phase II trials of patients with advanced bladder carcinoma can be influenced by patient population [23], thus, it is notable that modified MVAC still had a clinical benefit in our patients with poor prognosis (visceral metastasis, 49%; ECOG performance status 2, 20%). Thus, a significant objective response could be achieved with application of modified MVAC in selected patients with advanced urothelial cancer.
The modified MVAC used in this study was more tolerable than standard MVAC. Thrombocytopenia commonly observed in standard MVAC was rare, and non-hematological toxicities found in standard MVAC (mucositis and alopecia) did not occur. In addition, cisplatin-induced grade 3 or 4 renal toxicity was not apparent.
Conclusion
In conclusion, cisplatin-based modified MVAC chemotherapy is a tolerable and active salvage treatment for patients with advanced UC after failure of GC. Although this study is a retrospective chart review of a few cases, MVAC is a valuable treatment option in selected patients with a stable physical status and adequate renal function after progression of GC treatment.