Korea implemented a national healthcare system (National Health Insurance, NHI) in 1977, which expanded to the entire Korean population in 1989. By 2016, the NHI covered 97.1% of the population [1]. The top three causes of death in Korea are cancer, heart disease, and cerebrovascular disease [2]. Copayments for hospital fees for these diseases or rare diseases are 5% as compared with 20%-30% for other diseases. Because of this support from the government and a well-developed cancer screening policy, which started in the 1980s, the cancer survival rate in Korea has been increasing and the cancer incidence rate has been decreasing since 2011 [3].
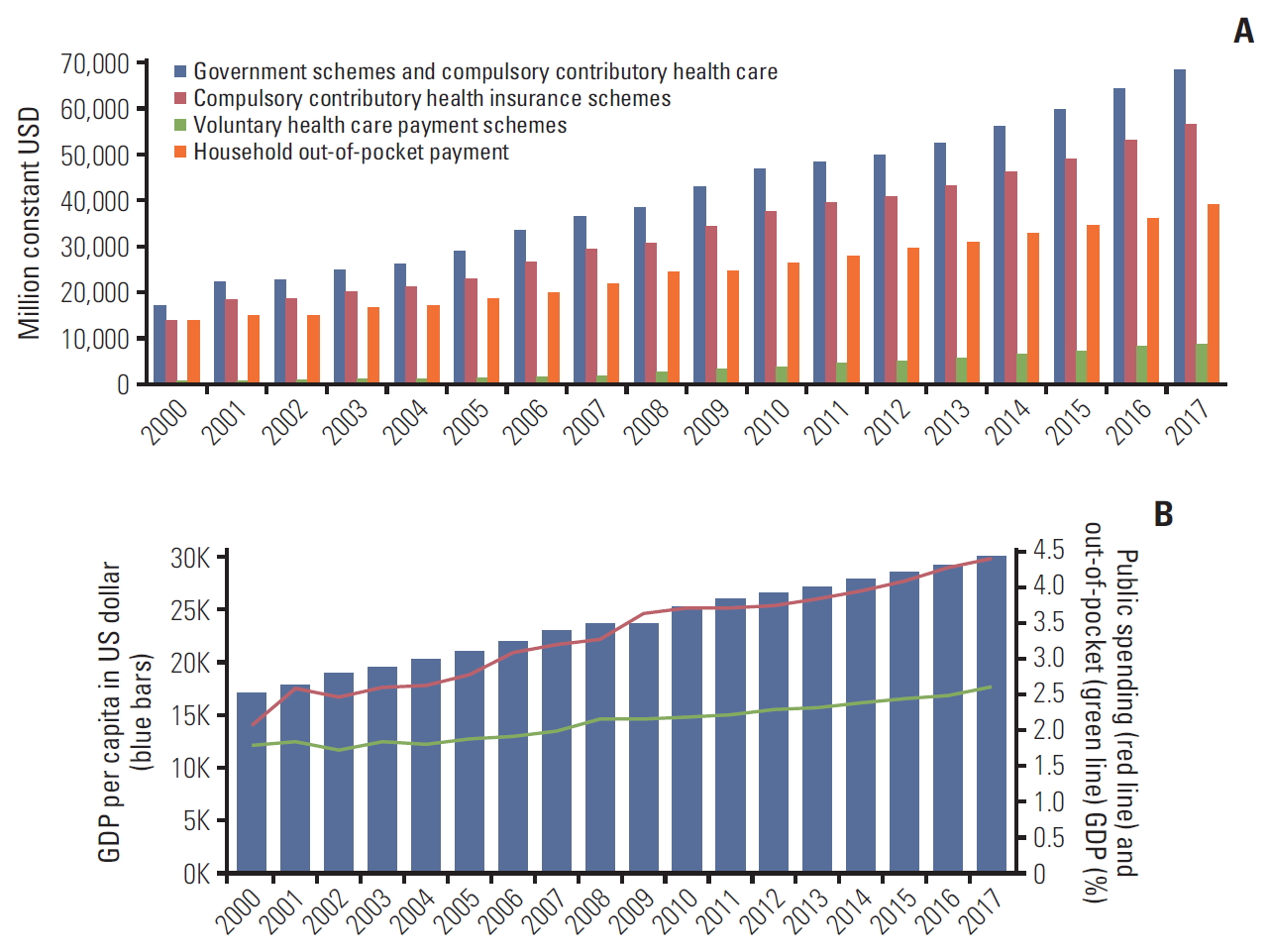
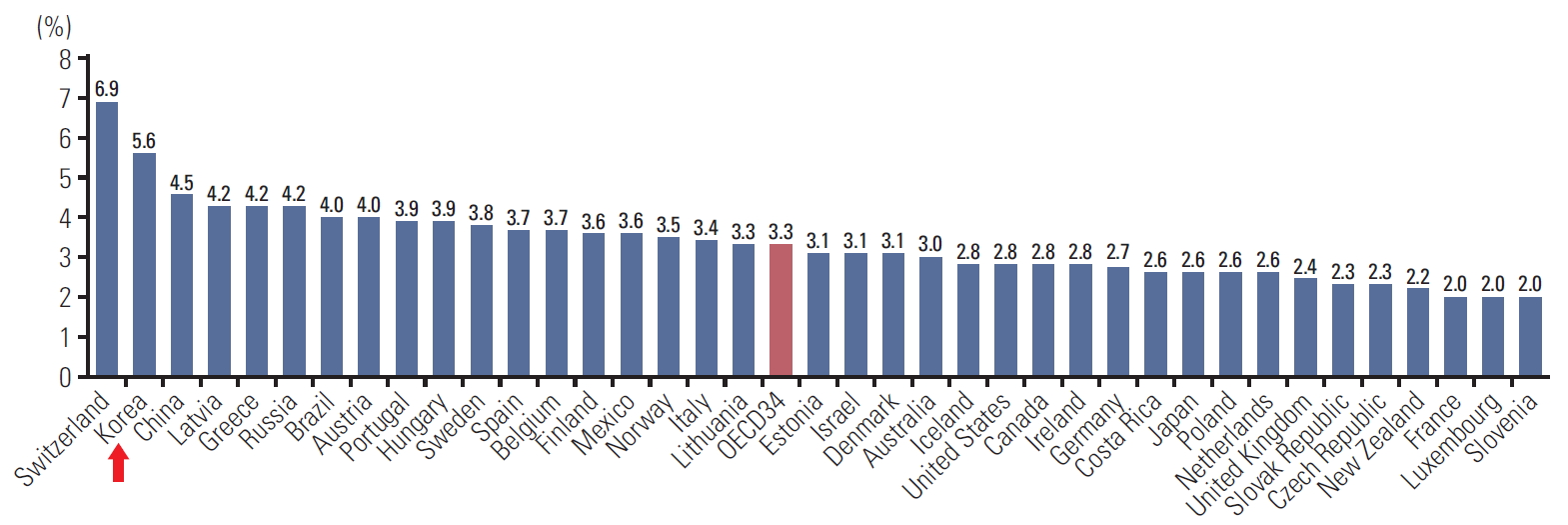
Government healthcare expenditure is rapidly rising in Korea, having increased from 5.4% of the gross domestic product in 2008-2013 to 7.3% in 2013-2018 and further to 8.1% in 2019; this is only slightly lower than the average in other Organization for Economic Co-operation and Development (OECD) countries, which is 8.8% [4]. The portion of healthcare costs borne by the patient is also high in Korea (33.7% in 2017) relative to that in other OECD countries (Fig. 1A). As the gross domestic product has increased in Korea, so too has public spending on health expenditure (Fig. 1A) [5,6]. However, out-of-pocket payments by patients have not decreased in proportion to this rise in public spending [6] (Fig. 1B). Out-of-pocket expenses are the costs of medical care that are not covered by insurance and that one pays for on their own. Fig. 2 shows out-of-pocket spending relative to final household consumption in 2017. Although Korea is classified as a high-income country by the World Bank, outof-pocket spending is still high, at 34% of healthcare expenditures compared to an average of 22% in other high-income countries [4]. Across OECD countries, an average of about 3% of total household spending is on healthcare-related goods and services, with Korea ranking near the top (5.6%, red arrow in Fig. 2) [4,7]. The share of household consumption spent on health care provides an aggregate assessment of the financial burden of out-of-pocket expenditures, which can overwhelm poor house-holds that have to pay for long-term treatment for chronic diseases such as cancer.
This phenomenon may be partly explained by the demand for many different types of treatment by patients, beyond standard care. The immediate availability of diverse private insurance products, which offer broad coverage of treatment costs, has accentuated this demand. There are two types of private insurance, fixed-payment insurance, and variable payment insurance. Unlike fixed-payment insurance, variable-payment insurance, which is sometimes also referred to as actual payment insurance, is basically a fee-for-service health plan that reimburses up to 90% of the medical expenditure as patients consume health-related services. Hence, many people in Korea have variable-payment insurance with or without fixed-payment private insurance. In 2017, 66% of people in Korea were covered by variable-payment insurance [8]. Small and medium-sized cancer care hospitals, which accommodate patients who are being treated or who have been treated with radiotherapy or chemotherapy, offer patients various supportive care services. The desires and needs of patients who want more supportive care are generally fulfilled by these services. However, patients are also offered alternative therapies, including mistletoe, selenium, high-dose vitamin C, and hyperthermia, for example, and these practices have been subject to extensive litigation between private insurance companies who want to pay less and patients who want greater coverage. In 2018, the Financial Supervisory Service (FSS) in Korea announced guidelines clarifying the necessary components of cancer care and stipulated their coverage as part of private health insurance [9]. The intention was to reduce future disagreement between patients and private insurance companies regarding indemnity payments.
In 2018, the number of patients who received government reimbursement reached 1,140,000 and the expenditure for cancer care was KRW 7.5 trillion or 24% of the total expenditure for the 12 most common chronic diseases [10]. This amount represents 9.6% of the total reimbursement reported by the NHI and the Health Insurance Review & Assessment Service (HIRA). However, it is doubtful whether the quality of cancer care is increasing in parallel with the escalating healthcare costs. As the costs of treatment and patient demand for services continue to escalate, it is clear that cancer care needs to be optimized. The key to optimizing care is to balance the provision of quality cancer care with sustainable costs. It is currently the duty of medical professionals to achieve this goal. They must set clear standards of care as well as educate patients and clinicians. It is not politicians or vendors who must set new standards of care, but medical professionals who can connect patient-oriented values and medical practice.
As a first step to achieving this goal, it is important to systematically measure the effects of treatment, and evaluate patient reported outcomes. Clinical practice should prioritize high-value care based on high-quality evidence. Good measures should be able to differentiate high-quality care from low-quality care, and should provide insight whether the healthcare providers support good practices. Also, an evaluation system should be able to incentivize higher-quality care by adopting alternative reimbursement mechanisms, if needed. The Korean government is primarily focused on expanding healthcare coverage for cancer and other diseases, while medical fees are fixed at low prices [11]. This generates pressure on health-care providers who need to balance costs and reimbursement. As a result, providers may prioritize high-frequency practices rather than high-value ones. Factors such as sta-ffing, interdisciplinary communication, and supportive infra-structure should also be considered when evaluating the outcomes that matter to patients [12]. Hence, a well-defined assessment system should be able to motivate clinicians to improve care delivery, not just press them to conform to strict reimbursement criteria.
This current situation in cancer care in Korea was identified as the foremost issue by the Korean Cancer Association (KCA), which led to the implementation of the nationwide ‘Right Decision in Cancer Care’ initiative. The United States National Quality Forum (NCF) on cancer made 10 recommendations to improve the quality of cancer care and correct problems in healthcare services. It called for major revisions to healthcare delivery, clinician education and trai-ning, and quality improvement in cancer care in the United States [13].
The KCA is composed of multidisciplinary specialists from various cancer-related fields [14]. Inspired by the Choosing Wisely Campaign in the United States, a task force was organized under the KCA Review Committee, and the idea to develop a nationwide campaign was approved by the KCA Board of Directors in May 2019. This accords with the global movement aimed at using medical resources more wisely and providing patients with the best outcomes by applying evidence-based, necessary treatments and encouraging the medical society to reduce low-value practice [15-18]. The initiative seeks to address several widespread problems associated with the underuse, overuse, or misuse of healthcare, and the authors call for dedicated efforts by clinicians towards education and training of the patients, and towards better health delivery, evaluation, and reimbursement for medical services.
Potential items to be included in the initiative were considered after reviewing the topics the Review Committee had covered over the last 3 years. The committee chose five items for the agenda, as follows.
(1) Do not delay palliative care in advanced cancer patients. Patients should ask how palliative care can be integrated with their course of treatment. In patients diagnosed with advanced cancer, end-of-life care should always be considered as part of the treatment plan. Sometimes cancer patients with advanced-stage disease are forced to choose between active anticancer therapy and palliative care services, but there is compelling evidence that early referral to palliative care even in the midst of active anticancer treatment significantly decreases the symptom burden and may also increase the survival of patients with advanced lung cancer [19]. Several prospective randomized clinical trials have evaluated early integration of palliative care with standard oncologic care, and the American Society of Clinical Oncology incorporated this into their clinical practice guidelines updated in 2017. They strongly recommended that pati-ents with advanced cancer should be referred to an inter-disciplinary palliative care team early in the disease course, alongside active anticancer treatment [20]. Additionally, patient protections and the Affordable Care Act in the United States brought forward end-of-life care as an important issue in cancer care, and asserted the necessity of making hospice service more broadly available to patients with serious illnesses including cancer [13,21].
(2) Pay attention to pain control in cancer patients. Patients should be aware of their pain symptoms and discuss these with medical staff. It is important to check whether cancer-related pain is managed appropriately. Both clinicians and patients should be educated to dispel misconceptions related to cancer pain. Although the pain score has been used as the “fifth vital sign” since 1996, many cancer patients suffer from significant pain due to underuse or avoidance of cancer-associated pain control. Pain was reported to affect up to 64% of cancer patients, and 43% of these patients felt that their pain control was inappropriate; many barriers to adequate pain control, including societal, regulatory, clinician, patient, and socioeconomic conditions have been identified [22,23]. Therefore, the policy for controlling cancer pain control should be comprehensive, entailing medical management, psychosocial support, education of the patient and caregiver, and interventional therapy, including radiotherapy.
(3) Do not use hyperthermia alone in treating cancer. If hyperthermia is proposed as a single treatment, ask your doctor how hyperthermia works in ameliorating symptoms or treating your cancer. Hyperthermia as a single treatment is not recommended for the treatment of cancer. In addition, hyperthermia does not have clinical effects as adjuvant therapy following surgery [24,25]. However, there is some clinical evidence supporting hyperthermia for locally advanced, unresectable solid tumors in combination with radiotherapy [26].
(4) Use brachytherapy appropriately for patients with uterine cancer. If you have uterine cancer or uterine cervical cancer, ask your doctor(s) if brachytherapy is needed in the course of treatment. For uterine cancer, brachytherapy should be used with or without external beam radiotherapy (EBRT), as appropriate. For cervical cancer, brachytherapy is an essential component of radiotherapy; the adoption of intensity-modulated radiotherapy or stereotactic radiotherapy instead of brachytherapy is associated with decreased survival rates in patients with cervical cancer [27,28]. For endometrial cancer, EBRT should not be routinely used as adjuvant radiotherapy in patients with early stage cancer if brachytherapy is considered adequate. EBRT is associated with a higher rate of pelvic organ complications, and is more time- and cost-intensive than brachytherapy [29]. Brachytherapy is an example of a high-value practice that is underestimated by health providers due to its low relative value unit and low medical price in Korea. Brachytherapy is currently available in a limited number of hospitals in Korea [30].
(5) Consult a medical specialist when considering travelling abroad for carbon ion particle therapy. If a patient enquires about carbon ion particle therapy, the clinician should refer the patient to an appropriate specialist in the field. Patients should avoid traveling abroad for carbon ion beam therapy without consulting a radiation oncologist, or if it is not recommended by a multidisciplinary tumor board that includes a radiation oncologist. There are many commercial agencies advertising for and private insurance companies selling insurance covering medical tourism in the absence of medical advice. For patients with disseminated cancer, medical tourism which requires long distance trip may be unnecessary and may even be harmful. It may also place the patient in a dangerous medical situation [31].
In conclusion, the launch of Korea’s nationwide ‘Right Decision in Cancer Care’ initiative highlights the current agenda for cancer care that should be discussed between physicians and patients, before any treatment decisions are made. Cancer survival and patient-defined quality of life should be used as one of the most important end-points to evaluate the quality of cancer care, and treatment costs should also be taken into consideration. Patients and physicians should work together to ensure high-value care is provided and that healthcare resources are used wisely. Healthcare providers and physicians need to adhere to evidence-based practices, and policy makers should establish tools capable of accurately measuring value-oriented healthcare and incentivizing high-value practices [32]. This article, as a first step in the ‘Right Decision in Cancer Care’ initiative, presents the initial five items on the agenda; however, the initiative should be expanded to provide more opportunities to correct and to prevent problems of underuse, overuse, and misuse of finite cancer care resources, and to finally improve the quality of cancer care in Korea.