INTRODUCTION
Colorectal cancer is the fourth most common malignant disease worldwide. In Korea, colorectal cancer makes up 11.2% of all the malignant disease and it is the fourth most frequent cause of cancer-related death (1). The incidence and mortality of this disease has increased in recent years (2). As a result, many topics concerned with colorectal cancer have been investigated. On the basis of those studies, it has been possible to predict the precise survival of colorectal cancer patients and to determine their prognosis.
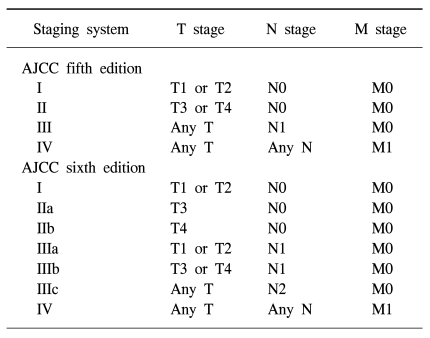
The prognosis is related to the depth of tumor penetration into the bowel wall and the presence of both regional lymph node involvement and distant metastasis. These variables are incorporated into the various staging systems that have been recommended by Cuthbert Dukes and modified by Kirklin et al and Astler and Coller (3~5). In 1987 (6), the International Union Against Cancer (UICC) and the American Joint Committee on Cancer (AJCC) devised a worldwide taxonomy of cancer staging (TNM) based on the localized tumor characteristics, nodal involvement and the status of the metastatic implants (7). Since January 1, 2003, the sixth edition of the AJCC Cancer Staging Manual has been used to stage all the new cancer cases (8), and this has now become the standard (Table 1) (9).
However, it hasn't yet been determined whether the sixth edition AJCC staging system could be applied to Koreans, so we evaluated its value by performing retrospective analysis. The results will help us make a decision on whether the new system can be applicable to Korean clinical practice, and especially in the Youngdong district, which is the eastern coast area of Gangwondo.
MATERIALS AND METHODS
1) Materials
We identified and evaluated 376 patients who were pathologically diagnosed with colorectal cancer at the Gangneung Asan Hospital from September 1, 1996 through December 31, pathologic characteristics. 2003. Those patients who expired within a month after surgery and those who had double primary or appendiceal cancer were excluded. Finally, only 365 of the 376 patients were eligible for this study. The median follow up duration was 51.0±30.4 months (maximum duration: 120 months).
2) Tumor and disease characteristics
The data of the patients was evaluated and classified at presentation, including the stage at surgery. Each tumor stage was coded as described by the AJCC fifth and sixth editions according to the TNM stage (T1: tumor invades the submucosa, T2: tumor invades the muscularis propria, T3: tumor invades through the muscularis propria into the subserosa or into the nonperitonealized pericolic tissues, T4: tumor directly invades other organs or structures and/or perforates the visceral peritoneum, N0: no regional lymph node metastasis, N1: metastasis to one to three regional lymph nodes, N2: metastasis to four or more regional lymph nodes, M0: no distant metastasis, M1: distant metastasis) (Table 1). All the patients were assigned to both staging systems and then they were analyzed for survival. The cancer-specific data for each patient contained the tumor location (right colon, transverse colon, left colon, rectum), tumor grade (well differentiated, moderately differentiated, poorly differentiated, anaplastic or undifferentiated), specific histology (adenocarcinoma, mucinous, signet ring cell), and metastases at presentation.
3) Statistical analysis
The descriptive statistics were calculated, including the means and medians or the counts and percentages. Kaplan-Meier analyses were performed to determine the overall survival and 5-year survival for the stages defined by both the fifth and sixth edition staging systems. All statistical analyses used SPSS version 13.0 (SPSS for Windows, Advanced Statistics, Inc., Chicago). p values for the survival curves were determined from the Kaplan-Meier survival curves by using the log-rank test. Those p values less than .05 were considered statistically significant.
RESULTS
1) Patients characteristics
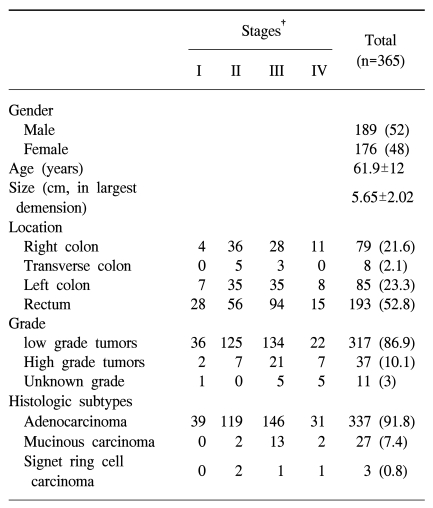
A total of 365 patients participated in this analysis. The total group consisted of 189 men (52%) and 176 women (48%). The median age for the cohort was 61.9±12 years. We described the baseline characteristics of all the enrolled patients in Table 2.
The anatomical location of the primary tumor was specified. Among the patients in the entire cohort, 79 (21.6%) had tumors in the right colon (cecum, ascending colon and hepatic flexure), 8 (2.1%) had tumors in the transverse colon, 85 (23.3%) had tumors in the left colon (splenic flexure, descending, sigmoid colon), and 193 (52.8%) had tumors in the rectum.
The tumor grade was categorized as low grade (well or moderately differentiated) and high grade (poorly differentiated, anaplastic or undifferentiated). Among all the patients in the cohort, 317 (86.9%) had low-grade tumors, 37 (10.1%) had high-grade tumors and 11 (3%) had tumors unknown.
The histologic subtype was classified as adenocarcinoma, mucinous adenocarcinoma and signet ring cell carcinomas. 337 patients (91.8%) had adenocarcinomas, 27 (7.4%) had mucinous adenocarcinomas, and 3 (0.8%) had signet ring cell carcinomas (Table 2).
Among the patients in the entire cohort, 185 (50.7%) had positive lymph nodes. The median number of biopsied lymph nodes was 23.6±18.4 (N0: 22.7±15, N1: 22.5±27.2, N2: 26±14). The median number of nodes that showed regional metastasis was 1.8±0.7 in N1; 11.2±9.7 in N2 disease. The AJCC and the International Union Against Cancer have recommended that a minimum of 12 lymph nodes have to be examined for proper staging. In this study, we followed this recommendation (10).
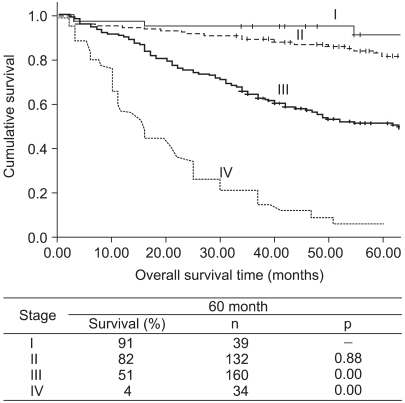
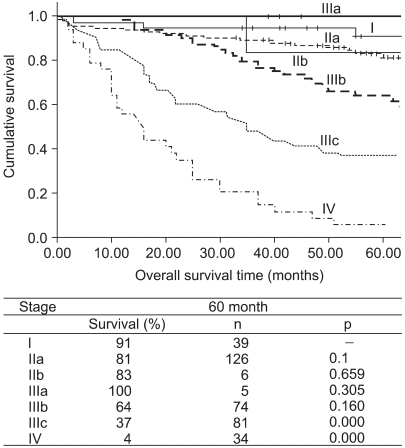
2) Survival according to the AJCC fifth and sixth edition staging
The overall 5-year survival for the entire cohort was 62%. According to the stages defined by the AJCC fifth edition system, the 5-year stage-specific survival was 91% for stage I, 82% for stage II, 51% for stage III and 4% for stage IV. By the revised system, it was 91% for stage I, 81% for stage IIa, 83% for stage IIb, 100% for stage IIIa, 64% for stage IIIb, 37% for stage IIIc and 4% for stage IV. The survival analysis for the cohort with using the fifth edition staging system is shown in Fig. 1, and that with using the sixth edition is shown in Fig. 2. According to the fifth edition staging system, the differences in the 5-year stage-specific survival rates were statistically significant among the three groups (stage II vs stage III and stage III vs stage IV, p<.0001), but not between stage I and II (p=0.08). According to the sixth edition staging system, the three groups (stage IIIb vs. stage IIIc and stage IIIc vs. stage IV) showed statistically significant differences (p<.001) but the others didn't. The 5-year survival rates were much better for the patients with stage IIIb (64%) than stage IIIc (37%) (p<.001).
In addition, we evaluated other potential prognostic factors (the grade, histologic subtypes and tumor location) that could be incorporated into a new colon cancer staging system. But the very small sample size of some variables (IIb, IIIa, signet ring cell adenocarcinoma in the histological subset, transverse colon in the anatomical subset) made it difficult to compute statistics.
DISCUSSION
Stage is the strongest predictor of survival for patients with colorectal cancer. Numerous different staging systems have historically been employed, but a single international system is required to ensure there is a common language for cancer that is understood by clinicians of all specialties. The TNM staging system has been widely used.
For the last two decades, agreement on cancer staging between the AJCC and the UICC has created a staging vocabulary that has been used to quantify the tumor burden of patients with colorectal cancer (6). The fifth edition system separated patients suffering with colon cancer into four stages, with somewhat wide spacing between the survival curves and particularly around stages II and III. The sixth edition of the AJCC Cancer Staging Manual brought about refinements of colorectal cancer staging, and these refinements were based on large data sets from the National Cancer Data Base (NCDB) (8,11); stages II and III were stratified into two and three subsets, respectively, and some of the gaps in the survival curves were filled in. Although the increased stratification of a staging system did not necessarily lead to different treatments (e.g., stage IIIa versus IIIb), it does provide important prognostic information that may help future clinical trials and improve the evidence-based literature.
Under the AJCC sixth edition staging system, it is interesting that stage IIIa shows rather better survival compared with that of stage IIb disease, which was similarity observed in our study (stage IIIa: 100% vs stage IIb: 84%). This finding may reflect the fact that adjuvant chemotherapy is recommended for stage III colon cancer patients, but not for the stage II patients (12). The three groups (stage IIIb vs. stage IIIc and stage IIIc vs. stage IV) showed statistic significance (p<.001), but the others didn't. So, we couldn't tell if the prognosis can be more precisely gauged by the revised 6th AJCC staging system. Yet we showed that the 5-year survival rates were much better for patients with stage IIIb disease (64%) than for the patients with stage IIIc disease (37%) (p<.001). Larger scale studies are needed for further improvements.
Our study has several potential limitations. First, the results are based on a small population. Moreover, the number of enrolled patients from stage IIb (n=6) to IIIa (n=5) was small, so this may have caused failure to produce statistical significance between each stage (except stage IIIb vs. stage IIIc and stage IIIc vs. stage IV, p<.001). But when compared with a previous large study, their 5-year survival rates for each stage are similar to ours except for stage IIb (72.2% vs 83%) and IIIa (83.4% vs 100%) (13). These findings may reinforce the reliability of this study. Second, the subjects were limited to only one hospital's inpatients. Although a single hospital's data was used, the data may well represent the Yongdong district. The patients who are diagnosed with cancer at the other hospitals in Yongdong have a strong tendency to visit Gangneung Asan Hospital to confirm the diagnosis and receive medical treatment afterwards (14). Third, we had difficulty in collecting the organized treatment data, including that on chemotherapy, radiotherapy and the pattern of treatment failure, which can not be overlooked. Fourth, we evaluated survival for colon and rectal cancer separately, but the results were short of statistical power due to the small study population for these two maladies.
CONCLUSIONS
This work is one of the trials that has evaluated the new AJCC sixth edition staging system for colorectal cancer. We observed that stage IIIb disease had better survival than stage IIIc disease. Yet we couldn't confirm that this new staging system is relevant in Korean clinical practice. Therefore, further study that's based on a larger scale (both colon and rectal cancer) and more refined cancer registry data that includes the treatment data is required to proceed, so that we can confirm the propriety of the new staging system in Korean medical practice.