INTRODUCTION
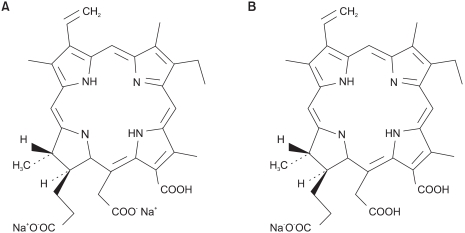
PDT is a novel treatment modality, which produces local tissue necrosis with laser light following the prior administration of a photosensitizing agent (1~4). Photosensitizers are applicable for the treatment of cancer as well as nontumoral diseases, such as psoriasis (5), bacterial and viral eradication (6,7), and for tumor detection (8). During the last several years, a whole range of dyes, such as Photofrin (USA, Canada), Photoscan (Germany), HPD (China), Photogem (Russia), Benzoporphyrin derivative (Canada), 5-aminolevulenic acid (ALA, Europe and USA) and Aspartate chlorine E6 (Japan), to name but a few, have been used as photosensitizers for a wide range of malignant tumors and non-malignant diseases (9~18). The disadvantages of using photosensitizers are poor tumor selectivity and prolonged photosensitization, which have yet to be overcome. Therefore, the application of PDT still remains limited due to the limited penetration of light in tissues, the chances of photosensitization of normal tissues and photosensitivity of the skin, which can last for 4~6 weeks after treatment (19,20). Recently, Radachlorin®, a derivative of the well-known water soluble green pigment chlorophyll α, has been shown to be a promising PDT sensitizer, and was first introduced as potential drugs by E. Snyder in 1942 (21). Radachlorin® as a drug substance represents an aqueous solution of three chlorins, including sodium chlorin e6 (90~95%) as the major ingredient, which is used as a carrier and solubilizing ligand (Fig. 1A), sodium chlorin p6 (5~7%) (Fig. 1B), and a third chlorin, which can not be disclosed (1~5%), both as pharmacogenic ingredients (Online at www.radapharma.ru). Thus, Radachlorin® (Fig. 1) is a complex natural photosensitizer as a drug accumulating and efficiently destroying tumors upon irradiation (662 nm). It has maximal tumor uptake 3~5 h post injection, with a high tumor-to-tumor tissue ratios and a clearance period of about 24~48 h (21). However, there have only been a few studies on the PDT effects of Radachlorin® in cervical cancer, although there have been several studies on Chlorin e6, which is a major component of Radachlorin®. Therefore, in this study, the PDT induced antitumor effects of Radachlorin® were evaluated in cervical cancer cells and an animal model.
MATERIALS AND METHODS
1) Photosensitizer
The Radachlorin® was purchased from the RADA-PHARMA group (RADA-PHARMA Co, Ltd., Moscow, Russia), which was stable in solutions at 0±8℃ in the dark.
2) Cell culture conditions
A mouse lung cancer cell line of TC-1 cells, which was derived from primary epithelial cells of C57BL/6 mice cotransformed with HPV-16 E6 and E7, as well as c-Ha-ras oncogenes (from Cancer Research Center, Seoul National University, Korea), were cultured on RPMI 1640 media (Gibco BRL, Rocksville, MD) supplemented with 10% fetal bovine serum (FBS) (Gibco BRL). Streptomycin/penicillin (Gibco BRL), L-glutamine (Gibco BRL), 2.2 mg/ml sodium bicarbonate (Sigma, St. Louis, MO) 0.4 mg/ml G418 disulfate (Duchefa, Netherlands) were added to the culture medium and the cells maintained at 37℃ in a 5% CO2 humid environment.
3) Immunization of mice
The female C57BL/6 mice (6~8 weeks old) were purchased from DaeHan Biolink (Daejon, Korea), and maintained under pathogen-free conditions. A TC-1 tumor animal model was established as previously reported (22). Briefly, 0.1 ml PBS suspension (3×106 cells/ml) of TC-1 cells was injected subcutaneously into the belly of the mice using a syringe. After the cancer cells had made a tumor size of 9 mm, the TC-1 cell implanted mice were then either i.v. or i.p. injected with 40 mg of Radachlorin®/kg of body weight (b.w.), respectively, and PDT performed.
4) PDT
The PDT was carried out using a laser apparatus generated by a diode (Won-PDT D662, Won Technology, Daejeon, Korea) equipped with high power laser diode module, with a built in temperature control system, optical fiber bundle and fiber test module. The wavelength was set at 662±3 nm. The duration of the light irradiation, under PDT treatment, was calculated taking into account the empirically found effective dose of light energy in J/W.
5) Radachlorin® uptake by TC-1 cells in vitro
TC-1 cells were inoculated into 6 well plates, with cover glasses, in a volume of 2 ml (5×104 cells/well) for a stationary culture. Twenty-four hours later, Radachlorin® (2.5, 5, 10, 20 and 50µg/ml) was added in a volume of 2 ml. After a predetermined time, the Radachlorin® solution was discarded; the TC-1 cells were washed twice with PBS and fixed with 1% paraformaldehyde. The cells were then washed again with distilled water, the cover glasses removed from the 6 well plates and mounted on slide glass. Confocal microscope (MRC 1024, Bio-RAD, Hercules, CA) measurements were performed at emission and excitation wavelengths of 545 and 600 nm.
6) MTT assay
TC-1 cell lines were inoculated into a 96-well, flat-bottomed microplate at a volume of 100µl (2×103 cells/well) for a stationary culture. Twenty-four hours later, the medium was removed, and the cultures washed three times in PBS. Various concentrations (0, 2.5, 5, 10 and 20 cg/ml) of Radachlorin® were then added in a volume of 100µl/well. Three or 12 h later, the Radachlorin® solution was discarded, the cultures washed a further three times with PBS and medium added to a volume of 100µl/well. The cultures were then subjected to laser irradiation (12.5 or 25 J/cm2), followed by the MTT assay to evaluate their sensitivity to PDT (Radachlorin®). For the MTT assay, 20µl of MTT reagent (5 mg/ml) was added to each cell culture well and cultured for 4 h. 200µl of DMSO was added to the culture, shaken for 10 min and the absorbance measured with an ELISA-reader at 570 nm. Measurements were performed for 6 days after the laser irradiation. Samples were assayed in triplicate, and the mean used as the measured value. The amount of Radachlorin® was also compared with the cancer cell lines.
7) Inhibition of TC-1 tumor growth in vivo
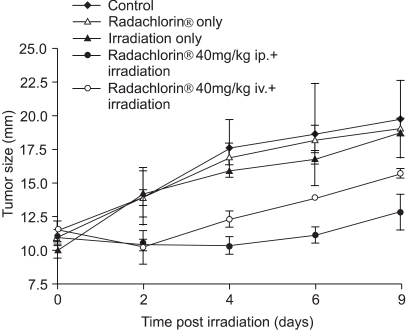
Animals were randomized into four groups (ten animals in each group): (◆) control (untreated); (Δ) Radachlorin® only; (▲) irradiation only; (○) Radachlorin® 40 mg/kg b.w. intravenous (i.v.) injection and irradiation; (●) Radachlorin® 40 mg/kg b.w. intraperitoneal (i.p.) injection and irradiation. The TC-1 cell implanted mice were either i.v. or i.p. injected with 40 mg of Radachlorin®/kg of b.w., respectively. The photodynamic treatment was carried out 24 h after the drug administration using 662 nm radiation from a diode laser. A power density of 2 W/cm2 and irradiation time of 150 sec was used. The tumor sizes were evaluated for 9 days by measuring two perpendicular diameters with calipers, and the tumor size calculated based on the average dimensions. The tumors were removed on the days indicated, and frozen to -70℃ until required for analysis.
RESULTS
1) Observation of Radachlorin® uptake by TC-1 cells
Fig. 2 shows the confocal microscopy of TC-1 cells after 24 h exposure to various concentrations of Radachlorin®. TC-1 cells were seen to contain Radachlorin®, which was excited to emit red to a confocal microscope. The luminescence of each cell was higher, in a Radachlorin® dose dependent manner (A-F). The Radachlorin® in the TC-1 cells showed no cytotoxicity, even with a higher concentration of 50µg/ml (data not shown).
2) Intracellular localization of Radachlorin®
It is important to determine the biological mechanism of action of a drug; therefore, the intracellular distribution of Radachlorin® was determined in TC-1 cells. The intracellular localization of TC-1 cells after 12 h incubation with 5µg/ml of Radachlorin® was measured by confocal microscopy (Fig. 3). The fluorescence was emitted from well-defined spots in the cytoplasm, and diffused fluorescence seen in the entire cytoplasm. The fluorescence micrographs suggested association of with the plasma membrane.
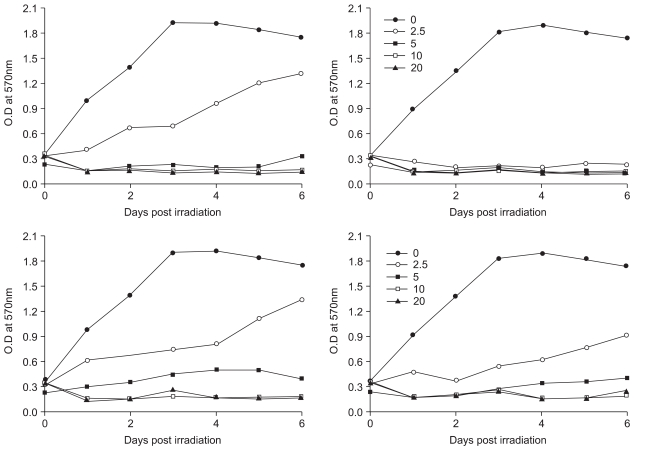
3) Antitumor effect of PDT using Radachlorin® in vitro
The efficacy of cell damage after PDT with Radachlorin® was further quantified by the MTT assay. The results of the experiment with TC-1 cells are shown in Fig. 4 (A-D). TC-1 cells incubated with various concentration of Radachlorin® and irradiated with laser showed significantly reduced cell viability with increasing light dose (B). However, when TC-1 cells were incubated with 2.5µg/ml of Radachlorin® for 3 h, and then irradiated with 25 Jcm2, the cell viability increased compare to the other Radachlorin® dosed cells (A). At the lowest light dose, 12.5 J/cm2, this experiment induced an increased cell viability when Radachlorin® was dosed at 2.5µg/ml and incubated for 3 and 12 h (C & D). Even though with a lower light dose exposure (12.5 J/cm2); the cell viability was significantly lower with an exposure time of Radachlorin® of 24 h than with 3 or 12 h (data not shown). Therefore, the optimal experimental drug dose of Radachlorin® seems to be 2.5µg/ml for 3 h or 12 h, with irradiation of 12.5 or 50 J/cm2, against TC-1 cells.
4) Measurement of Photodynamic effects in vivo
The antitumor activity of PDT using Radachlorin® in C57BL/6 mice with TC-1 tumors was determined, as shown in Fig. 5. In the Irradiation and Radachlorin® only group, the tumor sizes increased over the time period. It was observed that the control group, which showed a linear increase in tumor size over the time, was similar. The PDT only group showed no cytotoxicity in the TC-1 tumor lesions. Radachlorin® itself also had no toxicity on mice (data not shown). In the PDT using Radachlorin® treatment group, when the C57BL/6 mice with TC-1 tumors were PDT irradiated using 40 mg of Radachlorin®/kg b.w. (i.p.), the tumor size was significantly reduced compared to the other experimental and PDT using 40 mg of Radachlorin®/kg b.w. (i.v.) groups. PDT with an i.p. injection of Radachlorin® group showed improved antitumor effects over those with an i.v. injection.
DISCUSSION
Radachlorin® has recently been shown to be a promising PDT sensitizer (23), with a report showing the photodynamic effect on novel chlorin e6 derivatives, including Radachlorin®, on a single nerve cell (24). The study demonstrated that Radachlorin® was a most potent photosensitizer, comparable with Meso-[tetrakis(m-hydroxyphenyl)]chlorin (mTHPC), a well-known photosensitizer (24). In this study, TC-1 cells were shown to contain Radachlorin® in a dose dependent manner, which did not affect the viability of cells compared with the values of non-Radachlorin incubated cells (data not shown). Diffused fluorescence was found in the entire cytoplasm. Localization of Radachlorin® up take by TC-1 cells was not studied in detail in the present study. A previous report has shown that localization of intracellular photosensitizer depends on the lipophilicity and amphiphilicity of the photosensitizer (25). When incubated with cells, molecules of the photosensitizer were first adsorbed onto the plasma membrane and then penetrated into the cells. Hydrophilic photosensitizers that cannot cross the plasma membrane penetrated into the cell by means of pinocytosis, with taken up into the vesicles, endosomes and lysosomes. Following photodamage of these organelles, photosensitizers enter the cytosol and sensitize different cellular structures. Our data showed that Radachlorin® was seen to be adsorbed into the entire cytosol.
In a previous study, a PC12 (pheochromocytoma) cell line and the MTT test were used for in vitro assays, and laser light of 662 nm for Radachlorin® at the doses of 50 J/cm2 was irradiated (21). Radachlorin® did not show toxicity on the PC12 cell lines without irradiation, except with very high concentrations. Thus, in vitro Radachlorin® is a less toxic and more efficient photosensitizer upon irradiation than the other photosensitizers available (www.radapharma.ru). Our data also demonstrated that Radachlorin® treatment showed no cytotoxicity on TC-1 cells (data not shown), which supports the findings from previous experiments (21). In the irradiation treated group without Radachlorin® the accumulation also had no antitumor effect on mice with TC-1 tumors, as shown in Fig. 5. Therefore, these data suggested that Radachlorin® and PDT should be used together for the efficient destruction of the tumor lesions in TC-1 tumors. Pharmacokinetics and biodistribution studies (21, www.radapharma.ru) in mice have shown that maximal tumor accumulation of Radachlorin® was achieved 5 and 0.5 h after intraperitoneal and intravenous administrations, respectively. The highest contrast with Radachlorin® was observed at 18 h after the intraperitoneal administration with the tumor-to-muscle ratio of about 32, and tumor-to-skin ratio of about 44. The full clearance period was been found to be 48 h after the intraperitoneal administration via all routes of administration, a very important point as regards the problem of skin phototoxicity (23). Therefore, Radachlorin® shows excellent characteristics for use with PDT (21). Our preexperimental data were similar; however, the results have not been shown in this paper. Our data also support the advantageous use of Radachlorin® with PDT (data not shown). in vivo experimental data (Fig. 5) suggest that the PDT with an i.p. injection of Radachlorin® group showed an improved antitumor effect over those with an i.v. injection. This was probably due to the mechanisms of Radachlorin® accumulation via the two injection routes being different, but these remain for further study. Further study will be critical to follow up the tumor size and tumor survival in the long term, more than 60 days, to obtain a conclusive result.